
Translate this page into:
Dietary pattern in Adult Patients with Acute Stroke in South India: A Case-Control Study from a Tertiary Care Center in Hyderabad
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background and Objective:
Diet plays a crucial role in the occurrence of stroke. But very few studies have so far been conducted with focus on this aspect of acute stroke in India. The objective of the study was to identify the dietary pattern in patients with acute stroke in South India.
Materials and Methods:
Patients with first-ever acute stroke (ischemic and hemorrhagic) admitted between June 2017 and November 2017 were enrolled and compared with age- and sex-matched controls. Information was collected using a pro forma.
Results:
Out of 293 acute stroke patients, 150 were enrolled and compared with 150 controls. The mean age was 52.3 ± 12.6; years 112 (74.6%) patients were male. The majority of them were on traditional diet that included a daily intake of rice (98.6%) and pulses (40.6%). Hypertension (73.3%) was the major vascular risk factor for stroke (P < 0.0001). Significant differences were observed in risk factors such as diabetes (P < 0.0001), smoking (P = 0.0001), alcohol use (P = 0.0017), and heart disease (P = 0.0002), when stroke patients were compared with controls. Stroke patients reported a lower intake of green leafy vegetables (P = 0.0001; odds ratio [OR] 0.17), roots and tubers (P = 0.0016; OR 0.21), and fruits (P = 0.0022; OR 0.29). There was at the same time a higher intake of red meat products (P = 0.04; OR 2.41), organ meats (P = 0.0093; OR 4.35), fried snacks (P = 0.0038; OR 2.01), and pickles (P = 0.04; OR 1.81) although the data suggested lesser consumption of prawn and crab (P = 0.04; OR 0.55) and water (P = 0.0001 OR 4.59) among stroke patients. Higher consumption of fruit juices (P = 0.0008) and junk foods (P = 0.03) was observed in young stroke patients (age ≤45 years) whereas the intake of chicken (P = 0.03) and alcohol (P = 0.0001) was observed to be more among men than among women.
Conclusion:
Majority of stroke-afflicted patients in South India consume white rice and dal. There is lower intake of water, green leafy vegetables, and fruits and higher consumption of red meat, organ meat, and pickles among stroke patients.
Keywords
Dietary intake
food frequency
India
stroke

INTRODUCTION
Stroke is an important cause of mortality and morbidity among middle-income groups in countries like India. The prevalence rate of stroke in India is 84–262/100,000 in its rural areas and 334–424/10,000 in urban areas.[1] Hence, lifestyle modification can play a significant role in the primary and secondary prevention of stroke.
Diet plays a key role in the development of stroke through several mechanisms. Higher intake of carbohydrate-rich diet (starch, sugars, refined carbohydrate, and sweetened beverages) causes obesity,[2] raised fasting glucose, and risk of developing diabetes mellitus Type II that turn out to be risk factors for stroke. Higher consumption of dietary saturated fatty acid (SFA) is associated with stroke mortality in both sexes.[3] However, Framingham study has shown that intake of total and monounsaturated fat is associated with reduced risk of ischemic stroke.[4] Higher salt intake is associated with increased blood pressure and causes fibrosis in the heart, kidney, and arterial tissue.[5] Intake of green and yellow vegetables, fruits, fibers, and whole grain is protective against ischemic stroke.[6] Consumption of red meat has also been positively associated with blood pressure, the incidence of hypertension, metabolic syndrome, and inflammation.[78] Daily consumption of three or more cups of tea (green or black) is associated with a 21% lower risk of stroke compared to those who consume <1 cup/day.[9]
However, the resources concerning dietary pattern in stroke-afflicted patients in India are limited, and the only study, undertaken in Northwest India, suggested a higher consumption of milk and milk products and lower consumption of fruits and fruit juices among stroke patients.[10] Wide regional variability was also documented in the dietary pattern. The objective of the present study was to identify, by taking into account certain dietary components, the dietary pattern in South Indians admitted with acute stroke, by comparing them with healthy controls. To the best of our knowledge, this is the first study ever to identify and evaluate the dietary pattern in stroke patients from South India.
MATERIALS AND METHODS
Study design
This was a prospective case– control study and included patients with a diagnosis of first-ever acute stroke (ischemic and hemorrhagic) admitted to the Department of Neurology from June 2017 to November 2017 at ESIC Super Speciality Hospital, Hyderabad. Stroke was defined as an acute onset of focal neurological deficit and was confirmed by computed tomography scan or magnetic resonance imaging of the brain. Ischemic stroke was confirmed by a neurologist. Venous infarcts and Subarachnoid hemorrhage were excluded from the study. All patients were prospectively included in the ongoing register of patients with acute ischemic stroke at our hospital. Patients of stroke were matched (1:1) by age and sex with healthy controls. Dietary habits in stroke patients and healthy controls were assessed using a food frequency questionnaire that contained a list of 55 food items. The details collected were carefully examined and recorded by a qualified, expert dietician of our hospital.
Participants
Out of the 293 stroke patients, 150 patients with a diagnosis of acute stroke (ischemic and hemorrhage) were included in the study. Patients with prior history of stroke were excluded from the study. Those patients/relatives who were not willing to respond to the dietary questionnaire and those patients diagnosed with subarachnoid hemorrhage, venous infarct, and nonatherosclerotic vasculopathy were excluded from the study. Stroke patients were matched with 150 healthy controls [Figure 1]. Healthy individuals were those who visited the hospital for a routine health checkup and attendees of outpatient department and patients suffering from headache, musculoskeletal pain, and backache. Further, healthy individuals who were not on any dietary modifications were included in the study group as controls.
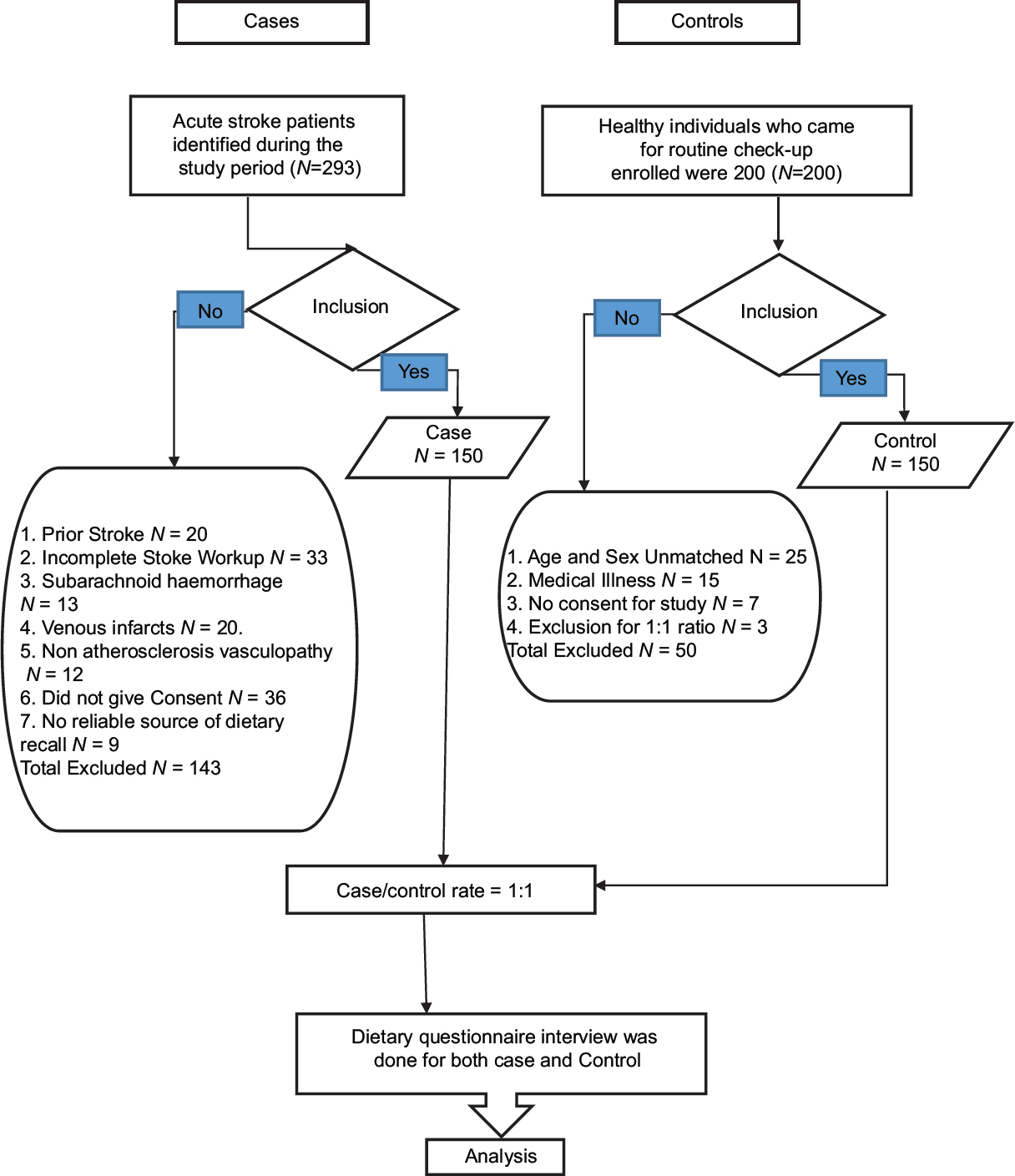
- Consort of flowchart
Information regarding reliable variables in the study, comprising demographic details, vascular risk factors and comorbid illnesses, type of stroke, questionnaire for selected dietary components, and water intake were collected using a structured pro forma. General information included the respondent's age, sex, weight, height, occupation, and type of stroke. Information regarding medical history of diabetes mellitus, hypertension, heart disease, prior stroke, migraine, hormonal therapy, and any other medical illness was collected. Habitual history, if any, of smoking, alcohol use, or tobacco chewing was also included. It was a 1-month recall of diet consumed and also its quantity. Depending on the type of food consumed, the quantity was measured as handful of rice, number of chapatti, liter of water, and teaspoon (tsp) of salt, sugar, oil, and pickles.
Participants were inquired about the frequency of consumption (daily, weekly, monthly, or rarely) of each food item and its quantity. Food categories included cereals, pulses, dairy products, vegetables, fruits, meat and meat products, fish, egg, fats and oils, sugars and jaggery, sweet items, fried snacks, junk foods and bakery items, salt and pickles, and carbonated beverages. The dietary questionnaire sought details on the frequency of intake of water and the consumption (daily, weekly, twice or thrice in a week, and monthly) of major food items such as cereals (rice, wheat, and jowar), whole grain, milk and milk products (tea, coffee, milk, curd, and buttermilk), and saturated fats (ghee, butter, dalda/vanaspati); type of oil (sunflower, groundnut, coconut, palm, mustard, olive, rice brain, cotton, and vegetable oil) consumed per day, per week, per month; daily, weekly, and monthly intake of fruits, fruit juices, snacks, biscuits, vada/puree, Chinese foods, junk foods such as noodles and fried rice; consumption of poultry products (egg, chicken), meat and meat products (mutton, pork, beef, and organ meat), seafoods (fish, prawn, crab) daily, per week, twice or thrice monthly. Organ meat included intake of liver, brain, spleen, and heart of chicken, mutton, beef, and pork; intake of sweets (sweet dishes, sugars, and jaggery), salts (1/2 tsp), pickles (1/2 tsp), papads, and groundnut and coconut chutney; information was gathered on the frequency of use of beverages (beer, whiskey, gin, rum, arrack) and cool drinks [Questionnaire 9.1]. Dietary data for stroke patients and healthy controls were entered simultaneously. Dietary questionnaire was answered by the patient himself/herself. However, in cases where the patient's response was inhibited due to the impact of stroke, a close relative was assigned to do it. The consent of the patient/relative was taken initially, and on completion, the respondent was required to sign at the end of the pro forma.
Statistical analysis
Data obtained in the study were subjected to statistical analysis with SPSS (version 18.0, IBM). Bivariate analysis was done using 2 × 2 Fisher's exact test for significance. A two-tailed P < 0.05 was considered as statistically significant. The odds ratio (OR) was calculated to know the risk of exposure to and consumption of a particular food. All confidence intervals (CIs) were set at 95%. Multivariate analysis included adjustment for age and sex.
Ethics statement
The information obtained in this study was collected prospectively with the approval of the local ethics committee. All patients and healthy participants gave their informed consent before their inclusion in the study.
RESULTS
Out of the 293 acute stroke patients, complete nutritional analysis was performed in 150 individuals admitted with first-ever acute stroke (ischemic and hemorrhagic). These patients were matched with 150 healthy controls. Of the 150 stroke patients, 118 patients had ischemic and 32 patients had a hemorrhagic stroke.
The mean age of stroke patients was 52.4 ± 12.6 years (range 20–80); 112 (74.6%) patients were males and 38(25.3%) patients were females. The mean age of healthy controls was 52.1 ± 12.5 years (range 19–80) with gender similar to stroke patients. Forty-seven (31.3%) patients had early occurrence of stroke (age ≤45 years) while 103(68.6%) patients had old age stroke. Significant differences were perceived in vascular risk factors that included diabetes, hypertension, heart diseases, smoking, and alcohol consumption in stroke patients compared to healthy controls [Table 1].
| Stroke patients (n=150), n (%) | Controls (n=150), n (%) | P | |
|---|---|---|---|
| Male | 112 (74.6) | 112 (74.6) | 1 |
| Female | 38 (25.3) | 38 (25.3) | 1 |
| Diabetes | 48 (32) | 0 | <0.0001 |
| Hypertension | 110 (73.3) | 3 (2) | <0.0001 |
| Heart diseases | 13 (8.6) | 0 | 0.0002 |
| Smoking | 62 (41.3) | 29 (19.3) | <0.0001 |
| Alcohol use | 84 (56) | 56 (37.3) | 0.0017 |
| Tobacco chewing | 25 (16.6) | 15 (10) | 0.1256 |
The majority of patients were on traditional diet that included a daily intake of rice (98.6%) and pulses (40.6%). There was no significant difference in macronutrient intake (cereals, pulses) between stroke-afflicted patients and healthy controls. We observed a lower intake of green leafy vegetables (P = 0.0001, CI = 0.06–0.43), roots and tubers (P = 0.0016, CI = 0.07–0.57), and fruits (P = 0.0022, CI = 0.13–0.64) in stroke patients than in controls. About 94.6% stroke patients consumed tea daily (94.6% stroke cases vs. 90% controls; P = 0.19). Stroke patients also reported a higher intake of red meat (P = 0.04, OR 2.41), organ meat (P = 0.0093, OR 4.35), and a lesser intake of prawn and crab (P = 0.04, OR 0.55) compared to healthy controls [Table 2].
| Food items | Stroke patients (n=150), n (%) | Controls (n=150), n (%) | P | OR (95% CI) |
|---|---|---|---|---|
| Cereals | ||||
| Rice/day | 148 (98.6) | 147 (98) | 1 | 1.51 (0.24-9.17) |
| Wheat/week | 106 (70.6) | 98 (65.3) | 0.38 | 1.52 (0.94-2.44) |
| Jowar/week | 48 (32) | 43 (28.6) | 0.6 | 1.17 (0.71-1.91) |
| Pulses/day | 61 (40.6) | 75 (50) | 0.13 | 0.68 (0.43-1.08) |
| Whole pulses/week | 5 (3.3) | 11 (7.3) | 0.19 | 0.43 (0.14-1.2) |
| Milk products | ||||
| Curds (/day) | 66 (44) | 76 (50.6) | 0.29 | 0.76 (0.48-1.2) |
| Butter milk (/day) | 33 (22) | 48 (32) | 0.06 | 0.59 (0.35-1.00) |
| Ghee (/week) | 20 (13.3) | 29 (19.3) | 0.21 | 0.64 (0.34-1.19) |
| Butter (/week) | 1 (0.6) | 2 (1.3) | 1.0 | 0.49 (0.04-5.53) |
| Tea (/day) | 142 (94.6) | 135 (90) | 0.19 | 1.97 (0.81-4.80) |
| Vegetables and fruits | ||||
| Green leafy vegetables (/day) | 6 (4) | 29 (19.3) | 0.0001* | 0.17 (0.06-0.43) |
| Roots and tubers (/week) | 5 (3.3) | 21 (14) | 0.0016* | 0.21 (0.07-0.57) |
| Other vegetables (/day) | 127 (84.6) | 130 (86.6) | 0.74 | 0.84 (0.44-1.6) |
| Fruits (/day) | 9 (6) | 27 (18) | 0.0022* | 0.29 (0.13--0.64) |
| Fruit juices (/day) | 23 (15.3) | 31 (20.6) | 0.29 | 0.69 (0.38-1.25) |
| Meat and meat products | ||||
| Chicken (/week) | 89 (59.3) | 96 (64) | 0.47 | 0.82 (0.51-1.3) |
| Mutton (/week) | 64 (42.6) | 70 (46.6) | 0.56 | 0.85 (0.53-1.34) |
| Fish (/week) | 35 (23.3) | 45 (30) | 0.23 | 0.71 (0.42-1.18) |
| Pork/beef (total consumption) | 20 (13.3) | 9 (6) | 0.04* | 2.41 (1.05-5.48) |
| Organ meats (/week) | 16 (10.6) | 4 (2.6) | 0.0093* | 4.35 (1.42-13.3) |
| Prawn/crab (total consumption) | 29 (19.3) | 45 (30) | 0.04* | 0.55 (0.32-0.95) |
| Egg (/week) | 118 (78.6) | 120 (80) | 0.8 | 0.92 (0.52--1.61) |
| Sugar and jaggery | 124 (82.6) | 134 (89.3) | 0.13 | 0.56 (0.29-1.11) |
*Significant. OR: Odds ratio, CI: Confidence interval
Regarding proportional consumption of miscellaneous foods, stroke patients reported higher consumption of fried snacks (P = 0.0038, OR 2.01), pickles (P = 0.04, OR 1.81), and saturated fats (P = 0.04, OR 2.17) compared to healthy participants. The salt intake was 1 tsp/day in majority of both cases and controls. While 18.9% of the patients consumed pickles daily, 23.58% controls consumed pickles twice/thrice in a week [Table 3].
| Foods | Stroke patients (n=150), n (%) | Controls (n=150), n (%) | P | OR (95% CI) |
|---|---|---|---|---|
| Deep fried snacks (/week) | 92 (61.3) | 66 (44) | 0.0038* | 2.01 (1.27-3.19) |
| Biscuits (/week) | 76 (50.7) | 97 (64.7) | 0.01* | 0.56 (0.35-0.89) |
| Vada/puri (/month) | 95 (63.3) | 90 (60) | 0.68 | 1.15 (0.72-1.83) |
| Sweets (/week) | 23 (15.3) | 34 (22.7) | 0.14 | 0.61 (0.34-1.11) |
| Chinese/junk foods | 53 (35.3) | 42 (28) | 0.21 | 1.40 (0.86-2.29) |
| Salt (/day) | 146 (97.3) | 143 (95.3) | 0.54 | 1.78 (0.51-6.23) |
| Dalda/vanaspathi | 22 (14.6) | 11 (7.3) | 0.04* | 2.17 (1.01-4.65) |
| Pickles (/week) | 125 (83.3) | 110 (73.3) | 0.04* | 1.81 (1.03-3.18) |
| Papad (/week) | 76 (50.6) | 86 (57.3) | 0.29 | 0.76 (0.48-1.20) |
| Ground nut chutney (/week) | 98 (65.3) | 108 (72) | 0.26 | 0.73 (0.44-1.19) |
| Cool drinks (total consumption) | 102 (68) | 104 (69.3) | 0.90 | 0.93 (0.57-1.53) |
| Alcohol (beer/whisky/rum)/day | 47 (31.3) | 10 (6.7) | 0.0001* | 6.38 (3.08-13.2) |
| Less intake of water (≤1 L)/day | 40 (26.7) | 11 (7.3) | 0.0001* | 4.59 (2.25-9.37) |
| More intake of water (2-3 L)/day | 110 (73) | 139 (92.7) | 0.0001* | 0.21 (0.10-0.44) |
*Statistically significant. OR: Odds ratio, CI: Confidence interval
While consumption of alcohol was higher in stroke patients (P = 0.0001, OR 6.38), water intake (<1 L) was found to be low (P = 0.0001, OR 4.59); healthy participants had higher intake of water (2–3 L) than stroke patients (P = 0.0001, CI = 0.10–0.44) [Table 3].
In subgroup analysis of stroke patients based on the type of stroke, ischemic stroke patients had a lower consumption of fruits as compared to hemorrhagic cases (P = 0.015) [Table 4]. Further analysis, based on gender, disclosed that men had higher consumption of chicken (P = 0.03) and alcohol intake (P = 0.0001) when compared to women. Younger stroke patients had higher consumption of fruit juices (P = 0.0008) and junk foods (P = 0.03) when compared to an older stroke group (age >45 years) [Table 5]. Most of the fruit juices consumed by young stroke patients were not fresh juices but were tetra packs. Consumption of tender coconut water was found to be very less. Among Ischemic stroke, commonest location was in Capsulo-ganglionic region, while in Haemorrhagic stroke, thalamic bleed was predominate [Table 6].
| Food items consumed | Ischemic stroke (n=118), n (%) | Hemorrhagic stroke (n=32), n (%) | P |
|---|---|---|---|
| Water intake | |||
| <1 L/day | 31 (26.27) | 9 (28.12) | 0.82 |
| >2 L/day | 87 (73.2) | 23 (71.8) | 0.82 |
| Alcohol use/week | 53 (44.91) | 18 (56.25) | 0.3191 |
| Vegetables and green leafy vegetables/day | 107 (90.67) | 26 (81.25) | 0.203 |
| Fruits/week | 59 (50) | 24 (75) | 0.015* |
| Mutton/week | 49 (41.52) | 15 (46.87) | 0.68 |
| Rice/day | 116 (98.30) | 32 (100) | 1.00 |
| Wheat/day | 32 (27.11) | 7 (21.87) | 0.65 |
| Jowar/week | 39 (33.05) | 9 (28.12) | 0.67 |
| Pulses/day | 47 (39.83) | 14 (43.75) | 0.69 |
| Whole grains/week | 4 (3.39) | 1 (3.125) | 1.00 |
| Milk and milk products/day | 105 (88.98) | 28 (87.5) | 0.76 |
| Curds/day | 54 (45.76) | 12 (37.5) | 0.06 |
| Butter milk/day | 25 (21.18) | 8 (25) | 0.63 |
| Roots and tubers/day | 2 (1.69) | 3 (9.37) | 0.06 |
| Chicken/week | 65 (55.08) | 24 (75) | 0.04 |
| Fish/week | 27 (22.88) | 8 (25) | 0.81 |
| Pork/beef/week | 11 (9.32) | 2 (6.25) | 0.73 |
| Egg/week | 91 (77.11) | 27 (84.37) | 0.47 |
| Organ meats/week | 11 (9.32) | 2 (6.25) | 0.73 |
| Prawn/crab/week | 6 (50.84) | 1 (3.12) | 1.00 |
| Dalda/Vanaspathi/week | 4 (3.39) | 0 | 0.57 |
| Fruit juices/week | 14 (11.86) | 9 (28.12) | 0.048 |
| Snacks/week | 65 (55.08) | 18 (56.25) | 1.000 |
| Biscuits/week | 59 (50) | 17 (53.12) | 0.84 |
| Vada or puri/week | 31 (26.27) | 11 (34.37) | 0.38 |
| Sweets/week | 18 (15.25) | 5 (15.62) | 1.00 |
| Chinese or junk food/week | 7 (5.93) | 2 (6.25) | 1.00 |
| Cool dinks/week | 22 (18.64) | 12 (37.5) | 0.03 |
| Sugar and jaggery/day | 97 (82.2) | 27 (84.37) | 1.00 |
| Salt/day | 116 (98.3) | 30 (93.75) | 0.19 |
| Pickle/week | 89 (75.42) | 27 (84.37) | 0.347 |
| Papad/week | 62 (52.54) | 14 (43.75) | 0.428 |
| Ground nut and coconut/week | 77 (65.25) | 21 (65.62) | 1.00 |
*Statistically significant
| Foods consumed | Gender | P | |
|---|---|---|---|
| Male (n=112), n (%) | Female (n=38), n (%) | ||
| Vegetables and green leafy vegetables/day | 100 (89.28) | 33 (86.8) | 0.76 |
| Fruits/week | 58 (51.78) | 25 (65.78) | 0.18 |
| Fruit juices/week | 22 (19.6) | 12 (31.57) | 0.17 |
| Chicken/week | 72 (64.28) | 17 (44.73) | 0.03* |
| Mutton/week | 47 (41.96) | 17 (44.73) | 0.85 |
| Curd/week | 85 (75.89) | 26 (68.4) | 0.39 |
| Butter milk/week | 45 (40.17) | 18 (47.36) | 0.45 |
| Alcohol/week | 65 (58.03) | 6 (15.78) | 0.0001* |
| Foods consumed | Age group | P | |
| Young (<45 years) (n=47), n (%) | Old (>45 years) (n=103), n (%) | ||
| Vegetables and green leafy vegetables/day | 40 (85.1) | 93 (90.29) | 0.40 |
| Fruits/week | 29 (61.7) | 54 (52.4) | 0.37 |
| Fruit juices/week | 20 (42.55) | 16 (15.5) | 0.0008* |
| Chicken/week | 29 (61.7) | 60 (58.25) | 0.72 |
| Mutton/week | 18 (38.29) | 46 (44.66) | 0.48 |
| Curd/week | 35 (74.46) | 76 (73.78) | 1.0 |
| Butter milk/week | 16 (34.04) | 47 (45.6) | 0.21 |
| Alcohol/week | 22 (46.80) | 49 (47.57) | 1.0 |
| Junk foods/week | 7 (14.8) | 4 (3.88) | 0.03* |
| Snacks/week | 20 (42.55) | 59 (57.28) | 0.11 |
*Statistically significant
| Anatomic location of stroke | number n (%) |
|---|---|
| Ischemic stroke (n=118), n (%) | |
| Frontal | 6 (5.08) |
| Parietal | 11 (9.32) |
| Temporal | 3 (2.54) |
| Parieto-occipital | 8 (6.77) |
| Frontotemporoparietal | 13 (11.01) |
| Frontoparietal | 10 (8.47) |
| Capsuloganglionic | 20 (16.94) |
| Thalamus | 10 (8.47) |
| Basal ganglion | 12 (10.16) |
| Brainstem (pons/medulla) | 7 (5.93) |
| Cerebellum | 6 (5.08) |
| Genu and body of corpus callosum | 4 (3.38) |
| Semicentrum ovale + corona radiate | 8 (6.77) |
| Hemorrhagic stroke (n=32), n (%) | |
| Thalamic | 11 (34.37) |
| Capsuloganglionic | 9 (28.12) |
| Lobar | 5 (15.62) |
| Brainstem | 4 (12.5) |
| Cerebellar vermis | 3 (9.37) |
DISCUSSION
Diet and nutrition are vital to the prevention of stroke. Undoubtedly, dietary pattern is associated with risk factor management, and it has an independent role in stroke risk reduction. Indian cuisine comprises a wide range of regional and traditional varieties that are native to the Indian subcontinent. Food patterns may vary from region to region in view of the diversity in climate, soil type, culture, ethnic groups, and occupation. However, rice is the staple food in the majority of the South Indian states. Most South Indians consume cooked rice with dal (lentils) and the local cuisine usually includes pickles as an essential part of the meal. Both vegetarian and nonvegetarian foods are popular in Telangana. And Hyderabadi cuisine includes popular delicacies such as biryani, haleem, kheema, and baghara baingan.[11] Hyderabad diet is non vegetarian when compared to the vegetarian diet of North India.
Vascular risk factors such as diabetes, hypertension, heart diseases, smoking, and alcohol consumption were significantly higher in stroke patients compared to healthy controls. However, we could not establish a definite link between these vascular risk factors and diet. This might be due to the fact that a prospective healthy group with medical illness was excluded from the study.
Assessing the impact of nutrition level and dietary pattern of the food group would provide a greater insight into the role of nutrition in stroke risk [Table 5]. The present study assessed the dietary pattern in a series of first-ever acute stroke (ischemic and hemorrhagic) patients and healthy controls from a similar population (Telangana) at the same point of time. The significant differences observed in their diet pointed to lower consumption of green leafy vegetables, fruits, and roots and tubers and higher intake of red meat, organ meat, pickles, saturated fats, and fried snacks among stroke patients, compared to healthy controls. Differences were also observed in water and alcohol intake in stroke patients and healthy controls.
PREDIMED study has shown that the Mediterranean diet is associated with a lower risk of stroke, cardiovascular death, and myocardial infarction.[12] The Mediterranean diet is characterized by a high intake of olive oil (monounsaturated fat), fruits and vegetables, nuts and whole grains, moderate intake of fish and poultry, and low intake of dairy, red and processed meats, and sweets. The present study also demonstrates that an increased intake of red meat and saturated fat and lower intake of fruits and green leafy vegetables are associated with higher risk of stroke.
The staple food of Telangana state is rice. Almost all the patients and healthy controls consumed refined white rice in the form of cooked rice. While interviewing them, it was observed that in terms of quantity, stroke patients had higher consumption of rice than the control group, but we could not establish a significant difference between the groups as exact quantity of consumption was not measured. White rice-based foods are high in refined carbohydrates. A case–control study on Chinese population by Liang et al. reported white rice-based foods as being positively associated with risk of ischemic stroke. Further, the corresponding ORs of cooked rice, congee, and rice noodles were 2.73, 2.93, and 2.03, respectively.[13] Rice consumption was found to be equally high in both cases and controls, 98.6% and 98%, respectively. Among stroke (cases) patients, 32% had diabetes mellitus either detected recently or had prior medical history. This indicates that although both groups consumed rice, only stroke patients had diabetes, and hence, rice consumption alone was not associated with diabetes. In the present study, a combination of other factors such as alcohol consumption and carbohydrates’ intake (sweets and carbonated water) were observed to be higher in stroke patients, which would have led to stroke.
In our study, it was seen that the proportion of consumption of saturated fat was much higher in stroke patients when compared to controls. A meta-analysis study by Cheng et al. showed that a higher saturated fat intake was associated with reduced overall and fatal stroke risk in East Asians.[14] Similar finding was not noted in the present study. This discrepancy might be due to the change of region (South Asia), differences in dietary habits, inclusion of both ischemic and hemorrhagic groups, and the type of lipids consumed. It might also be due to the small sample size. For such a gross generalization of diet, a huge sample size is required. Studies on SFA intake and risk of ischemic stroke are inconsistent.[15]
A complex relationship prevails between alcohol consumption and stroke. One “standard” drink contains 14 g of pure alcohol, which is found in 12 ounces (360 ml) of regular beer (5% alcohol), 5 ounces (150 ml) of wine (12% alcohol), and 1.5 ounces (45 ml) of distilled spirits (40% alcohol). Regular consumption of alcohol ranging from moderate (3 or 4 drinks/day) to light (1 or 2 drinks) doses decreases the risk of ischemic stroke while heavy drinking magnifies the risk for both hemorrhagic and ischemic stroke.[1617] The threshold of alcohol effect in women (1–2 drinks) was lower than men (3–4 drinks).[17] Heavy drinkers are those who consume 15 or more drinks/week in males and 8 or more drinks/week in females. In our study, we observed higher intake of alcohol in stroke patients compared to control subjects, and majority of stroke patients consumed alcohol daily (heavy drinkers). Among stroke patients, there was a significant difference (P = 0.0001) in alcohol consumption pattern in women when compared to men. However, there were no significant differences observed between the young and the old stroke patients and between the types of stroke (ischemic and hemorrhagic).
Food-related healthier lifestyle was observed in healthy controls than in stroke patients. Regarding sodium intake, studies have demonstrated that reduced intake of salt is associated with primary prevention of stroke.[18] As per WHO guidelines, the recommended upper limit of sodium consumption per adult is 2 g/day or 1 tsp of salt. The present study found that although the majority of cases (70.6%) and controls (78.6%) consumed 1 tsp of salt per day, a higher proportion of cases (24.6%) consumed 2 tsp of salt when compared to controls (13.3%) which was statistically significant (P = 0.03). Further, the consumption of pickles per week was higher among stroke patients compared to controls (83.3% vs. 73.3%; P = 0.04). Hence, it is suggested that the high salt content in the pickles might be considered as higher sodium consumption per day that led to stroke.
In comparison with Western diet where there is higher consumption of fructose, soft drinks, meat, and saturated fat and lower consumption of fibers, fish, and vitamins,[19] the present study group from South India had lower consumption of soft drinks and fruits and higher consumption of meat, pickles, and polished rice. As per a North Indian study,[10] a majority of people in North India were vegetarians and consumed milk products while people living in Hyderabad region were nonvegetarians and consumed high-carbohydrate food.
Young stroke patients had significantly higher consumption of fruit juices compared to older stroke patients. The fruit juices consumed were tetra packs of mango (Maza, Fruity), guava, and apple. Packaged juices are not healthy when compared to whole fresh fruit juices. Consumption of tender coconut water was very less in the study group. Thus, consumption of packaged fruit juices have shown to be significantly associated with stroke in the young.
Limitations of the study include it being a case–control one and its exclusion of severe stroke patient who did not survive to participate in the study. The study lacked data on cholesterol levels, Vitamin B12, Vitamin D, folate levels, and quantity of each nutrient consumed by each group, thereby depriving the comparison of cholesterol levels and total calorie intake of the two groups. Another limitation of the study could be the inclusion of both types of stroke. Studies have established that low lipids are a risk factor for hemorrhagic stroke[20] while high lipids are a risk factor for ischemic stroke. Finally, the small sample size could have affected the possibility of establishing the significant differences in isolated nutrients.
To the best of our knowledge, the present study is the first of its kind that evaluates the association between dietary habits and acute stroke in South India. Low intake of fruits per week was observed in patients with hemorrhagic stroke compared to ischemic stroke patients. There were significant differences in the food habits of men with stroke compared to women stroke patients. Higher consumption of chicken and alcohol per week was observed in men than in women. Young patients with early occurrence of stroke consumed fruit juices and junk foods when compared to older patients. Thus, a healthy stroke diet rich in fresh whole fruits or juices, green leafy vegetables, lower consumption of salt and pickles, avoidance of organ meat, and higher water consumption in combination with traditional staple diet are the dietary modifications to be encouraged to prevent stroke in this region.
CONCLUSION
A majority of stroke patients from Hyderabad region consumed rice, mainly in the form of cooked rice with dal. There were major differences in dietary patterns between stroke patients and healthy controls. Lower intake of water, green leafy vegetables, and fruits and higher consumption of red meat, salt, organ meat, and pickles were observed in stroke patients. The high intake of these food items by a majority of stroke patients doesn’t necessarily translate into causality. Association may not always determine causation. High carbohydrate diet with low water intake was observed as a major dietary risk factor for stroke among the study group. Hence, a healthy dietary habit is a crucial factor in the prevention of risk of stroke in these populations.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors acknowledge the English grammatical revision by Dr. Anitha Prasannan, PhD English, retired Professor, SN College Kollam.
REFERENCES
- Carbohydrate intake, glycemic index, glycemic load, and dietary fiber in relation to risk of stroke in women. Am J Epidemiol. 2005;161:161-9.
- [Google Scholar]
- Dietary sodium, potassium, saturated fat, alcohol, and stroke mortality. Stroke. 1995;26:783-9.
- [Google Scholar]
- The Framingham heart study and the epidemiology of cardiovascular disease: A historical perspective. Lancet. 2014;383:999-1008.
- [Google Scholar]
- Salt intake, stroke, and cardiovascular disease: Meta-analysis of prospective studies. BMJ. 2009;339:b4567.
- [Google Scholar]
- Guidelines for the primary prevention of stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42:517-84.
- [Google Scholar]
- Relation of iron and red meat intake to blood pressure: Cross sectional epidemiological study. BMJ. 2008;337:a258.
- [Google Scholar]
- Meat intake and the risk of hypertension in middle-aged and older women. J Hypertens. 2008;26:215-22.
- [Google Scholar]
- Flavonoids, flavonoid-rich foods, and cardiovascular risk: A meta-analysis of randomized controlled trials. Am J Clin Nutr. 2008;88:38-50.
- [Google Scholar]
- Dietary patterns in stroke patients in Northwest India. Nutr Neurosci. 2013;16:288-92.
- [Google Scholar]
- Hyderabadi cuisine. Available from: https://en.wikipedia.org/wiki/Hyderabadi_cuisine
- Primary prevention of cardiovascular disease with a Mediterranean diet. N Engl J Med. 2013;368:1279-90.
- [Google Scholar]
- White rice-based food consumption and ischemic stroke risk: A case-control study in Southern China. J Stroke Cerebrovasc Dis. 2010;19:480-4.
- [Google Scholar]
- Can dietary saturated fat be beneficial in prevention of stroke risk? A meta-analysis. Neurol Sci. 2016;37:1089-98.
- [Google Scholar]
- Saturated fat consumption and risk of coronary heart disease and ischemic stroke: A science update. Ann Nutr Metab. 2017;70:26-33.
- [Google Scholar]
- Alcohol consumption and stroke: Benefits and risks. Alcohol Clin Exp Res. 1998;22:352S-8S.
- [Google Scholar]
- Moderate alcohol intake reduces risk of ischemic stroke in Korea. Neurology. 2015;85:1950-6.
- [Google Scholar]
- The mediating effect of the Mediterranean diet on the role of discretionary and hidden salt intake regarding non-fatal acute coronary syndrome or stroke events: Case/case-control study. Atherosclerosis. 2012;225:187-93.
- [Google Scholar]
- Prospective study of major dietary patterns and stroke risk in women. Stroke. 2004;35:2014-9.
- [Google Scholar]
- Blood lipid levels, statin therapy and risk of intracerebral hemorrhage versus ischemic vascular events: A prospective case control study from tertiary care centre of South India. Int J Res Med Sci. 2016;4:4857-61.
- [Google Scholar]
QUESTIONNAIRE
Questionnaire 9.1: Structured pro forma for dietary questionnaire including demographic profile and vascular risk factors
Topic: Dietary patterns in stroke patients – A hospital-based study
I. General Information
Name: _________________
Address: ______________________________________
Phone No: ________________________________
Type of stroke: Ischemic ◻ Hemorrhagic ◻
Sex: _______ (M/F)
Age: ____ Weight: ______kg Height: ______cm BMI: ______
Occupation: _____________________________ Monthly income________________
Intake of water per day_____ (1 L/2 L/3 L/____)
II. Medical History_____
1. Hypertension ◻ since when (no of years) ◻
2. Diabetes ◻ since when (no of years) ◻
3. Hyperlipidemia/dyslipidemia ◻ since when (no of years) ◻
4. Heart problems ◻ since when (no of years)◻
5. Old stroke ◻ year_____________
For female patients
6. Menopause ◻
7. Hormonal therapy ◻
8. Migraine ◻
9. Others ________ Specify_________________
III. Personal Habits
1) Smoking yes/no ◻
2) Chewed (paan, gutkha, khaini, and zarda) yes/no ◻
IV. Food frequency questionnaire
| Serial number: 1 | Cereals | Daily | Weekly once | Twice/thrice in a week | Monthly | Occasionally |
|---|---|---|---|---|---|---|
| 1.1 | Rice (polished/parboiled/brown) | |||||
| 1.2 | Wheat (whole/refined) | |||||
| 1.3 | Jowar | |||||
| 1.4 | Other cereals | |||||
| Serial number: 2 | Pulses | Daily | Weekly once | Twice/thrice in a week | Monthly | Occasionally |
| 2.1 | Red gram dhal/green gram dhal/black dhal/bengal gram/other* | |||||
| 2.2 | Whole red gram/whole green gram dhal/whole black dhal/whole bengal gram/other* | |||||
| Serial number: 3 | Milk and milk products | Daily | Weekly once | Twice/thrice in a week | Monthly | Occasionally |
| 3.1 | Milk/tea/coffee (whole/toned/skimmed/others__________) | |||||
| 3.2 | Curds | |||||
| 3.3 | Buttermilk | |||||
| 3.4 | Ghee | |||||
| 3.5 | Butter | |||||
| Serial number: 4 | Vegetables | Daily | Weekly once | Twice/thrice in a week | Monthly | Occasionally |
| 4.1 | Vegetables | |||||
| 4.2 | Roots and tubers | |||||
| 4.3 | Green leafy vegetables | |||||
| Serial number: 5 | Maat and meat products | Daily | Weekly once | Twice/thrice in a week | Monthly | Occasionally |
| 5.1 | Chicken (fry/curry) | |||||
| 5.2 | Mutton (fry/curry) | |||||
| 5.3 | Fish (fry/curry) | |||||
| 5.4 | Pork/beef (fry/curry) | |||||
| 5.5 | Egg (boiled/poached/omelette) | |||||
| 5.6 | Organ meats (liver, brain, kidney, etc.) | |||||
| 5.7 | Prawn, crab, others | |||||
| Serial number: 6 | Oil | Daily | Weekly once | Twice/thrice in a week | Monthly | Occasionally |
| 6.1 | Sunflower/groundnut/coconut/palm/mustard/olive oil/rice bran/cotton seed/soybean | |||||
| 6.2 | Dalda/vanaspathi | |||||
| Serial number: 7 | Fruits and fruit juices | Daily | Weekly once | Twice/thrice in a week | Monthly | Occasionally |
| 7.1 | Banana, apple, orange, mango, guava, grapes, papaya, pomegranate, sapota, watermelon, custard apple, sugarcane | |||||
| 7.2 | Fresh fruit juices | |||||
| Serial number: 8. | Snacks/sweets | Daily | Weekly once | Twice/thrice in a week | Monthly | Occasionally |
| 8.1 | Mixture, namkeen, khara boondi, samosa, bajji, bonda, Murukulu, sakinalu, etc. | |||||
| 8.2 | Biscuits (sweet/salt/bakery biscuits, Good Day, Marie) | |||||
| 8.3 | Vada, puri etc. | |||||
| 8.4 | Sweets | |||||
| 8.5 | Chinese/junk foods (noodles/fried rice) | |||||
| Serial number: 9 | Alcohol | Daily | Weekly once | Twice/thrice in a week | Monthly | Occasionally |
| 9.1 | Beer/whiskey/gin/rum, arrack others | |||||
| Serial number: 10. | Other beverages’ | Daily | Weekly once | Twice/thrice in a week | Monthly | Occasionally |
| 10.1 | Cool drinks | |||||
| Serial number: 11 | Sugar and jaggery | |||||
| Serial number: 12 | Salt (1 tsp/2 tsp) | |||||
| Serial number: 13 | Pickles (1 tsp/2 tsp) | |||||
| Serial number: 14 | Papad | |||||
| Serial number: 15 | Chutneys (coconut/ground nut) |




