
Translate this page into:
Clinical Characteristics of Essential Tremor in South India: A Hospital-Based Cohort Study
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
Essential tremor (ET) is the most common adult movement disorder. Classic ET is characterized by action tremor of hands (95% cases), and tremor involving other regions is less common. Recent studies have revealed a few patients exhibiting nontremor features that include cognitive disorders, tandem gait abnormality, mood fluctuations, olfactory abnormality, hearing impairment, and sleep disorders. Very few studies on ET have so far been conducted in India, and the present study is a pioneering attempt to evaluate the clinical characteristics of patients diagnosed with ET.
Materials and Methods:
A standardized assessment protocol was used to collect data. Diagnosis of ET was established using consensus criteria established by the Movement Disorder Society. Tremor Research Group Essential Tremor Rating Assessment Scale was used to evaluate tremor impact. The severity of hand tremor was assessed by Glass Scale, and cognitive function was assessed by Mini–Mental Status Examination.
Results:
Out of the 45 patients enrolled, 73.3% were male and 26.6% were female, with a mean age of 44 ± 15 years. Postural tremor was observed in all, followed by intention tremor in 9 and rest tremor in 6 patients. Tremor of the hand was identified to be most predominant (100%). Voice tremor was observed in 15 (33.3%) patients and head tremor in 12 patients (26.6%) who were all females. Leg tremor was observed in 12 patients (26.6% of patients) and tongue tremor in 6 (13%) patients. Baseline asymmetry of tremor was observed in 60% of patients and positive family history in 35% of patients. The most common nontremor feature was tandem gait abnormality (40%). Moreover, most of the patients had Glass Scale II.
Conclusion:
Baseline asymmetry of tremor and male predominance were observed in the study. While hand tremor was the most common form of tremor, tandem gait abnormality was the most common nontremor feature as observed in patients with ET.
Keywords
Clinical study
essential tremor
India

INTRODUCTION
Essential tremor (ET) is the most common tremor and adult movement disorder described,[12] and it is frequently associated with significant physical and psychosocial disabilities. Burresi was the first to use the term “essential tremor” in 1874, to describe patients with action tremor but without any other neurologic signs.[3] ET is generally characterized by action tremor of the upper limbs (95% of patients), and its manifestation in the head (34% of cases), face/jaw (7% of cases), voice (12% of cases), tongue (approximately 30%), trunk (approximately 5%), and lower limbs (approximately 30%)[4] is less common.
Several recent publications have established the presence of nontremor symptoms associated with ET. Moreover, these abnormalities include mild cognitive impairment,[567] apathy,[8] depression,[7] anxiety,[9] sleep disturbances,[10] reduced quality of life,[11] cerebellar dysfunction, and gait ataxia.[12] There are a few community-based studies that have established the prevalence of ET in India.[1314] The clinical characteristics of ET, which are considered to be twenty times more common than that of Parkinson's disease, have not been properly evaluated in India. We examined the clinical characteristics of patients diagnosed with ET and, to the best of our knowledge, this is the first-ever hospital-based study of ET with clinical analysis, from India.
MATERIALS AND METHODS
Study design
This is a single-center, hospital-based, cross-sectional study carried out over a period of 12 months from January 2017 to January 2018 at ESIC Super Specialty Centre, ESIC Medical College, Hyderabad, Telangana, India. In this study, we analyzed the clinical characteristics of ET.
Study sample
All patients suspected with ET visiting the hospital were screened for enrollment in the present study. Diagnosis of ET was established using the consensus criteria given by the movement study group.[15] Tremor Research Group Essential Tremor Rating Assessment Scale (TETRAS) was used to find the impact of ET during clinical examination.[16] The severity of hand tremor was assessed by Glass Scale.[17] Cognitive function was assessed through Mini–Mental Status Examination (MMSE).[18] Informed consent was obtained from eligible patients.
Data collection
Data were collected using a structured pro forma that sought information such as demographic details, medical history, use of tremorogenic drug, treatment history, family history, duration of tremor, results of neurological examination, location of tremor in the body, symmetric/asymmetric onset, type of tremor, nontremor features, response to alcohol, TETRAS score, Glass Scale, and MMSE scale. To study and assess the evolution of tremor over time, the patients were retrospectively inquired with specific questions such as when the tremor was first noted; whether there was difficulty in drinking from a glass using one hand, if so, the time when they first needed both hands to drink from a glass; and when exactly they required a straw. Whenever patients were unable to recall, all necessary information was gathered from their close relatives or caretakers. Computed tomography of the brain was done to rule out treatable structural lesion. Thyroid profile was done on every patient to rule out hyperthyroidism as the cause of tremor, in addition to the routine blood investigations. Appropriate clinical evaluation was done to look for bradykinesia, rigidity, postural instability, and resting tremor, in order to exclude Parkinson's disease.
Data analysis
Statistical analysis was done using SPSS software version 17, IBM software. Categorical variables were represented as counts and percentage and continuous variables as mean ± standard deviation. Fisher's test using 2 × 2 table was used to compare between continuous variables, and t-test was done to compare quantitative variables in the two groups. P ≤ 0.05 was considered statistically significant, and confidence interval was set at 95%.
RESULTS
In the present study, 45 patients comprising 33 (73.3%) males and 12 (26.6%) females diagnosed with ET were enrolled. The mean age was 44 ± 15 years. Hand was the most common location of tremor [Table 1].
| Body parts with tremor | n=45, n (%) | Males (n=33), n (%) | Females (n=12), n (%) | P |
|---|---|---|---|---|
| Hand tremor | 45 (100) | 33 (73.3) | 12 | <0.0001 |
| Voice tremor | 15 (33.3) | 12 (80) | 3 (20) | 0.002 |
| Head tremor | 12 (26.6) | 0 | 12 (100) | <0.0001 |
| Leg tremor | 12 (26.6) | 12 (100) | 0 | <0.0001 |
| Tongue tremor | 6 (13) | 6 (100) | 0 | 0.0022 |
Hand tremor, which was most common, was identified as postural tremor in 45 patients, followed by intention tremor in 9 patients and resting tremor in 6 patients. Baseline asymmetry of hand tremor was observed in 60% of patients. Baseline head tremor (HT) was observed in 7 patients (15.5%), who were all females, whereas 12 patients (26.6%) were found to have developed HT during the course of the disease. The most common nontremor feature was tandem gait abnormality (40%). The demographic and clinical characteristics of the patients in the study series are shown in Table 2.
| Characteristics of the study sample | n=45, n (%) |
|---|---|
| Definite ET | 30 (66.6) |
| Probable ET | 15 (33) |
| Age in years (mean) | 44±15 |
| Age at the first symptom (mean) | 40.6±15.4 |
| Men | 33 (73.3) |
| Total tremor score | 18.66±9.67 |
| Tremor duration (years), range | 3-15 |
| Mean tremor duration (years) | 6±2.81 |
| Postural tremor | 45 (100) |
| Intention tremor | 9 (20) |
| Rest tremor | 6 (13.3) |
| Cognitive impairment | 15 (33.3) |
| Tandem gait abnormality | 18 (40) |
| Baseline asymmetry | 27 (60) |
| Positive family history of ET | 16 (35) |
| Relief with alcohol | 8 (17.7) |
| Not tried alcohol | 37 (82.2) |
| Baseline head tremor | 7 (15.5) |
ET: Essential tremor
Holding a glass was the most difficult task observed in patients with ET. Out of the 45 patients, 25 (55.5%) were found to have Glass Scale score II (difficulty in drinking from a glass using one hand), 12 had Glass Scale Score III (when both hands were first needed to drink from a glass), and 8 patients had Glass Scale Score IV (when a straw was needed to drink). We found the following age distribution according to the Glass Scale scores: score I – 45 ± 7 years, Score II – 45 ± 15 years, Score III – 47 ± 17 years, and Score IV – 57 ± 14 years [Figure 1]. The mean time in years to reach each score was as follows: score II – 4 ± 3, Score III – 10 ± 5, and Score IV – 12 ± 8 years.
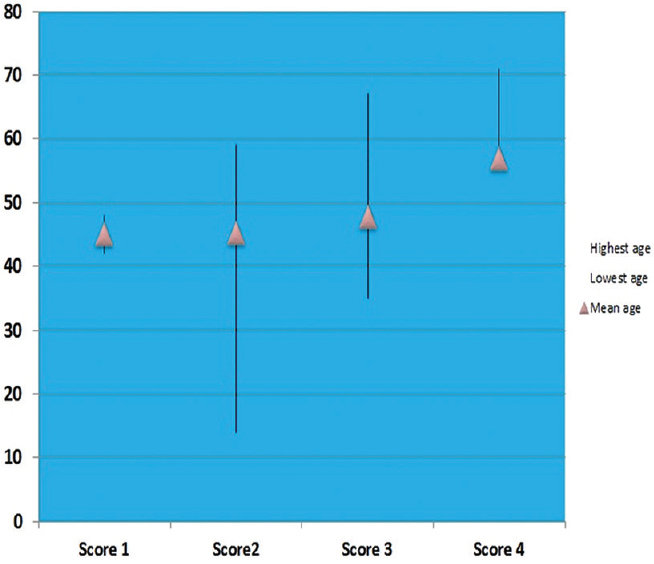
- Comparison of Glass Scale Score (X axis) with age in years (Y axis)
Further subanalysis was done using two groups of patients: patients in whom symptoms of ET first appeared before 40 years of age (n = 14; males: 14; mean age of onset = 24 ± 8 years) and patients in whom the symptoms appeared at 40 years or above (n = 31; males: 19;females: 12; mean age of onset = 51 ± 6 years). We found that all patients who experienced tremor at a younger age were male, while both sexes were affected in the older age group. Glass Scale Score II was reached at a mean age of 29 ± 10 years among the young and 54 ± 4 years among the older groups. We observed that patients who presented tremor at a younger age took 5 ± 3 years to reach Stage II, whereas patients with tremor at an older age took 3 ± 1 years [Figure 2] to reach the same stage. While the older age group took 8.5 ± 5 years, the young age group with early tremor onset took 3.37 ± 0.5 years to reach Stage III from Stage I. This difference was statistically significant (P = 0.012).

- Rate of progression of disease to Glass Scale Score II from Glass Scale Score I according to the age of onset of tremor
DISCUSSION
In the present study of 45 patients, we found that the prevalence of ET was more predominant in males, with a ratio of 2.7:1 (male: female). This ratio is higher when compared to the West (Spain) where in a study of fifty patients, male predominance of ET was noted at the ratio of 1.7:1.[19] Contrary to the results of a population-based study on Parsi community in India, our study did not reveal any female preponderance for ET.[13]
We found, as in earlier studies, a bimodal distribution of age in the onset of ET, with the lowest age of onset of ET being 9 years and the highest age being 59 years. The present study found that the prevalence of ET was significantly higher in the older age group (age >40 years) when compared to the young. This finding was similar to the results of previous studies conducted in India and worldwide. However, the mean age of patients with ET was much lower when compared to a Western study (44 vs. 72 years).[19]
HT was observed only in women in our study, indicating female preponderance, while both men and women were affected with hand tremors. We observed a lower percentage of patients of ET with HT (26.6%) when compared to a clinic-based sample study reported by Louis and Dogu[20] where they analyzed data from population-based and clinic-based case samples. In their study which included 583 patients with ET, the proportion of patients[20] with HT was 18% in population-based study from Turkey and New York, while the proportion of HT was 37.1% in the clinic-based sample study in New York.
Our study found that a higher proportion of men with ET had voice tremor and tongue tremor when compared to women (P = 0.002), whereas leg tremor was observed only in men (P < 0.0001). Tandem gait abnormality (40%) was the major nonmotor symptom in our sample of ET patients. A prior study reported by Fasano et al.[21] showed that the presence of intention tremor, a type of kinetic tremor, was a significant risk factor for balance and gait abnormalities in patients with ET. In our study, only 20% of patients with ET had intention tremor, thus implicating some other possible mechanism for gait abnormality. A higher age combined with cranial tremors, namely HT and voice tremor, has been described as the other possible mechanism for gait abnormality in previous studies. Our study result supports the previous studies pertaining to gait abnormality.
Presence of intention tremor in only 20% of cases with postural tremor indicates that all patients with postural tremor may not manifest intention tremor. Our findings were similar to those of a study reported by Sternberg et al.[22] In their study, they compared the postural tremor and intention tremor in patients with ET (fifty patients) with similar symptoms manifested by Parkinson's disease patients (fifty patients). It was found that intention tremor was present in 14 (28%) ET patients versus only 2 (4%) Parkinson's disease patients.
We found that patients with tremor onset at an older age progressed faster from functional Glass Scale Score I to Glass Scale Score II when compared with patients with tremor onset at a younger age of <40 years. This finding is similar to a previous study by Gironell et al.[19]
However, several limitations were observed in the present study. First, the study being a retrospective one, there might be low precision of data and limited knowledge of the progression of disease, especially with regard to Glass Scale Score IV. The second limitation observed was the rather short, 1-year duration of the study, and the third being the small sample size, as samples were collected on an outpatient basis, thus limiting predictive analysis and follow-up.
CONCLUSION
Although ET is most often considered as a disease of symmetrical presentation, baseline asymmetry was observed as the initial feature in majority of our patients. Appropriate clinical evaluation would definitely help to differentiate ET from Parkinson's disease, especially in cases where the onset of tremor occurs at an older age. ET is found to be more predominant among males. In the present study, HT was noted in females, which is similar to the results of Western studies. Tandem gait abnormality was observed to be the most common nonmotor feature in ET. Moreover, tremor onset at an older age was observed to progress faster.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Historical underpinnings of the term essential tremor in the late 19th century. Neurology. 2008;71:856-9.
- [Google Scholar]
- Action tremor of the legs in essential tremor: Prevalence, clinical correlates, and comparison with age-matched controls. Parkinsonism Relat Disord. 2009;15:602-5.
- [Google Scholar]
- Cognitive deficits in essential tremor consistent with frontosubcortical dysfunction. J Clin Exp Neuropsychol. 2008;30:760-5.
- [Google Scholar]
- Cognitive impairment in essential tremor without dementia. J Clin Neurol. 2009;5:81-4.
- [Google Scholar]
- Apathy in essential tremor, dystonia, and Parkinson's disease: A comparison with normal controls. Mov Disord. 2012;27:432-4.
- [Google Scholar]
- Sleep disturbances in essential tremor and Parkinson disease: A polysomnographic study. J Clin Sleep Med. 2015;11:655-62.
- [Google Scholar]
- Quality of life and personality in essential tremor patients. Mov Disord. 2006;21:1114-8.
- [Google Scholar]
- The balance and gait disorder of essential tremor: What does this mean for patients? Ther Adv Neurol Disord. 2013;6:229-36.
- [Google Scholar]
- Prevalence of essential tremor in the Parsi community of Bombay, India. Arch Neurol. 1988;45:907-8.
- [Google Scholar]
- Prevalence of essential tremor in the city of Kolkata, India: A house-to-house survey. Eur J Neurol. 2009;16:801-7.
- [Google Scholar]
- Consensus statement of the Movement Disorder Society on Tremor. Ad Hoc Scientific Committee. Mov Disord. 1998;13(Suppl 3):2-23.
- [Google Scholar]
- The glass scale: A simple tool to determine severity in essential tremor. Parkinsonism Relat Disord. 2010;16:412-4.
- [Google Scholar]
- “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189-98.
- [Google Scholar]
- Severity stages in essential tremor: A long-term retrospective study using the glass scale. Tremor Other Hyperkinet Mov (N Y). 2015;5:299.
- [Google Scholar]
- Isolated head tremor: Part of the clinical spectrum of essential tremor? Data from population-based and clinic-based case samples. Mov Disord. 2009;24:2281-5.
- [Google Scholar]
- Gait ataxia in essential tremor is differentially modulated by thalamic stimulation. Brain. 2010;133:3635-48.
- [Google Scholar]
- Postural and intention tremors: A Detailed clinical study of essential tremor vs. Parkinson's disease. Front Neurol. 2013;4:51.
- [Google Scholar]




