
Translate this page into:
Chance Fracture in an Unbelted Rear Seat Passenger
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Chance fracture occurs from flexion-distraction injury in motor vehicle road crash usually when the patient is on a seat belt. It is often associated with intra-abdominal injuries. We managed a 22-year old female unbelted rear seat passenger of a bus which was involved in a lone accident. We highlighted the possible mechanism of chance fracture in an unbelted passenger and satisfactory spinal stability on conservative care with neither internal nor external fixation.
Keywords
Chance fracture
conservative care
flexion-distraction injury
unbelted passenger

INTRODUCTION
Chance fracture is often results from flexion-distraction injury in motor vehicular collision. It occurs commonly in patients wearing seat belts; however, it has also been reported in unbelted individuals.[1234] There was a case report of a 21-year old man who slid down a flight of stairs and subsequently sustained chance fracture of the first lumbar vertebrae.[5] Chance fracture is an uncommon injury in an unbelted victim of lone motor vehicular accident.[4] We present an unusual mechanism of Chance fracture.
CASE REPORT
A 22-year-old right-handed female was referred to our unit on the April 14, 2014 with low back pain and difficulty with lifting both lower limbs of 4-h duration. She was an unbelted back seat passenger in an 18 seater bus which was involved in a lone accident. She was not ejected from the bus. There was no loss of consciousness, headache, seizures, vomiting, or bleeding from the craniofacial orifices. There was no history of numbness or weakness of the lower limbs. Initial care was at a nearby General Hospital and she was transferred to our center for further care. On examination, she was awake and alert with normal vital sign and the neurological examination. She had tenderness at T10 down to L5 and pelvic compression and distraction test was positive. The right lower limb was internally rotated and shortened while the left thigh was swollen and deformed. Urethral catheter was in situ draining clear urine. Examination of other systems was normal.
A clinical diagnosis of polytrauma with Frankel E thoracolumbar spine injury, right hip dislocation, and left femoral shaft fracture was made. Whole body CT scan showed L1 bony Chance fracture, fracture of L2 to L5 spinous processes [Figure 1], right hip fracture dislocation, and left femoral shaft fracture. She had closed reduction of the right hip fracture dislocation under sedation and open reduction as well as internal fixation of the left femoral shaft fracture under general anesthesia. The bony chance fracture was managed non-operatively; she was nursed flat on water bed for 8 weeks and subsequently had dynamic studies which showed satisfactory bony union [Figure 2]. There was no neurological deterioration and she was ambulated out of bed on Zimmer's frame. She was discharged home for follow-up at neurosurgical spine clinic.

- Computed tomography image showing L1 bony chance fracture
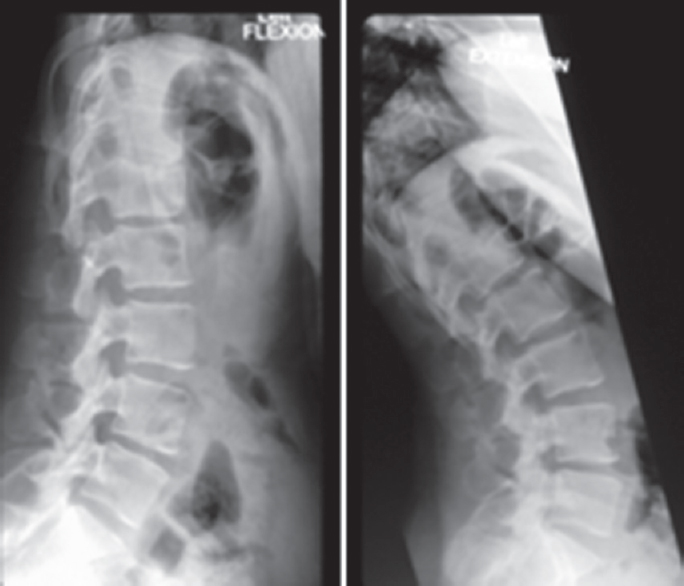
- Dynamic X-ray images showing satisfactory bone union
DISCUSSION
Chance fracture was first described in 1948.[6] It is a flexion-distraction injury resulting in compression injury to the anterior portion of the vertebral body and distraction injury to the posterior elements. This leads to a transverse fracture through the posterior portion of the vertebral body, pedicle, and spinous process. It is usually called seatbelt injury because of its association with seat belt. It is horizontal splitting of either the soft tissue or bone tissue or even both. The injury usually occurs at T12–L2 spinal levels usually in motor vehicle accident with the advent of lap seat belt.[35] It has also been reported in unbelted victim[4] and following a fall.[35] Intra-abdominal lesions are encountered in 30%–50% of Chance fracture patients.[12] The index patient was an unbelted victim of a lone motor vehicular accident and she had no clinical or radiologically confirmed abdominal injury probably because she was not on seat belt. The right hip dislocation and left femoral shaft fracture implied that the primary impact on both lower limbs was unbalanced probably leading to the twisting of the thoracolumbar spine and causing secondary spinal injury.[3] Neurological deficit occurs in about 1.4% but may be as high as 10.5% if diagnosis is delayed.[2] There was no neurological deficit in the index case, and the initial limitation of the lower limbs movement was due to the right hip fracture dislocation and left femoral shaft fracture. The radiologic findings may be subtle. Computerized tomograph is better than the routine X-ray in making the diagnosis because of its ability to remove overlapping osseous structures; however, the gold standard for the diagnosis of chance fracture is magnetic resonance imaging (MRI) scan. The MRI evaluation provides information on the integrity of the three columns of Denis, disc herniations, epidural hematoma and the spinal cord. We were unable to get the spine MRI for this patient because there was no functioning MRI machine in our hospital at the time.
Chance fracture is considered unstable and may be associated with significant instability which may worsen neurological function if not recognized.[7] It usually requires stabilization procedures either by internal or external fixation.[234] The treatment of this type of fracture depends on the severity of the injury regarding the neurological status and anatomical patterns of the fracture. Conservative treatment may be sufficient for bony lesions in patients without neurological deficits.[4] The ligamentous chance fracture usually requires operative care because of high failure rate of nonoperative care. Other indications for operative care include displaced fractures and progressive kyphosis on conservative care.[1] The absence of appropriate screws and functional intraoperative fluoroscopy prevented internal fixation with pedicle screws and rods. In addition, fracture of the lumbar spinous processes prevented the use of Adeolu et al. technique.[8]
CONCLUSION
Chance fracture is a flexion-distraction injury which usually occurs in a belted passenger during motor vehicle collision; however, it can also occur as a secondary injury when unbalanced forces acted on the lower limbs leading to twisting of the spine. A high index of suspicion and judicious use of imaging are crucial in diagnosis. Satisfactory bone union can be achieved without internal and or external fixation most especially in young patient with bony chance fracture.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Chance fracture in three brothers: A case report. J Bras Neurocirurg. 2013;24:322-6.
- [Google Scholar]
- The unusual chance fracture: Case report & literature review. Open Orthop J. 2013;7:301-3.
- [Google Scholar]
- Unique mechanism of chance fracture in a young adult male. West J Emerg Med. 2013;14:147-8.
- [Google Scholar]
- The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine (Phila Pa 1976). 1983;8:817-31.
- [Google Scholar]
- The technique of using rigid vertical strut and spinal process wire for posterior spinal stabilization. J Spinal Disord Tech. 2011;24:406-8.
- [Google Scholar]




