
Translate this page into:
Complete Femoral Nerve Transection with Sural Nerve Cable Graft in a 21-Month-Old Child
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Severe peripheral nerve injury occasionally requires urgent nerve grafting especially with significant separation of the proximal and distal ends of the injured nerve. Proper reinnervation to provide continued sensory and motor function is essential especially in the pediatric population. These patients would suffer lifelong disability without correction, yet have significantly improved regenerative capacity with prompt and effective management, making nerve grafts an ideal choice for complete nerve transection. This case report describes the successful sural nerve cable graft reinnervation of a transected femoral nerve in a 21-month-old male. This procedure was made difficult by severe trauma to the surrounding area with laceration of the femoral artery, significant separation of the femoral nerve ends, and the compact anatomy of such a young patient.
Keywords
Cable nerve graft
femoral nerve
nerve injury
pediatric
sural nerve

INTRODUCTION
Twenty million Americans suffer from peripheral nerve injury, most commonly in the upper limb because of trauma.[1] Severe nerve injury can cause sensory, and motor deficits are leading to neuropathic pain or paralysis of the affected limb.[2] Many injuries require surgery including the use of nerve grafts.
Nerve grafts are typically reserved for important motor nerve reconstruction using an expendable donor nerve and often provide many benefits. Nerve transfers minimize the distance over which a nerve must regenerate because it is closer to the target organ and is more specific.[3] With quicker nerve recovery, more rapid motor reeducation, and therefore, maximal functional recovery is possible.
With large nerve gaps that require bridging of the injury, autografts are the most reliable.[3] One of the most common forms of autografting is the cable graft, where multiple small caliber grafts are aligned in parallel to traverse a gap of transected nerve. Due to its location, dispensability, and size, the sural nerve is the most common nerve to use for cable grafting.[4]
CASE REPORT
A 21-month-old male was flown in from a rural town 200 miles away from the regional hospital. 4 h prior, a car fell on the patient, resulting in a crush injury with a large avulsion with partial laceration of the left femoral artery, and complete transection of the left femoral nerve. The initial presentation was of extensive trauma with 300 mL blood loss, acute respiratory failure, hemorrhagic shock, pelvic fracture, crush injury and 10-cm laceration with exposed bone, right proximal tibial fracture, and pulmonary contusion. On examination, his right leg had mild swelling and tenderness at the proximal tibia, with normal neurovascular function distally. On the left, he was able to dorsiflex and plantarflex the ankle and to flex the knee; however, there was no discernible quadriceps function.
The same day, he underwent surgery for a left femoral nerve reconstruction. Two sural nerve grafts, 10 cm and 12 cm in length, were carefully obtained from the child's right to retain the vasa nervorum. The edges of the nerve endings were cleaned, and the grafts were reversed to create proximodistal connections after loosening the femoral nerve ends to avoid tension, with graft lengths 10% longer than the defect length. Loose stitches were made with several bundle-to-bundle connections with sharp-to-sharp ends using 9-0 and 7-0 nylon suture with the aid of a microscope. Thorough antibiotic irrigation was applied, and a layer of venous blood was left to promote healing. The completed cable graft is shown in Figure 1. In addition, the femoral artery was repaired with end-to-end anastomosis and artery balloon dilations.
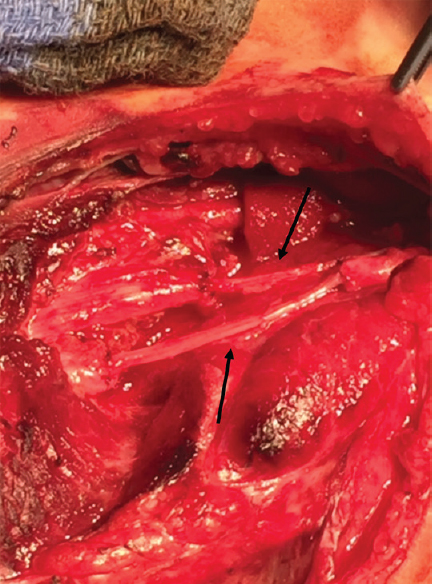
- The right sural nerve cable graft to the left femoral nerve transection. The two graft bundle locations are indicated with black arrows
Approximately 4 months postoperatively, the patient presented with normal tone in both legs with slight hyperextension of the left knee when walking and running. His recovery indicated satisfactory reinnervation of the territory of the affected femoral nerve, despite the use of a sensory nerve for motor repair.
This case is interesting due to the young age of the patient, the high degree of recovery, and the use of a relatively expendable sensory nerve with the necessary large diameter for motor repair. To the best of our knowledge, this is one of the youngest patients with a successful large-diameter cable nerve graft procedure.
DISCUSSION
Criteria for the choice of nerve graft donor as well as benchmarks for the assessment of reinnervation of denervated territory are described previously.[45] Our patient recovered full motor function in his quadriceps. It is interesting to note that though a sensory nerve was used for the repair; the patient regained full function. In general, it is recommended that mixed sensory-motor nerves are used for grafting or that the donor type is matched to the injured nerve.[56] The sural nerve is a relatively expendable nerve, and its successful use, in this case, is encouraging given the need for a large-diameter nerve.
Several studies have identified that key variables affecting the extent of peripheral nerve recovery after autograft procedures. Kallio and Vastamäki[7] concluded in their study assessing the median nerve autograft recovery of 132 patients that those who regain more functionality are on average younger than 54, have a graft length of <7 cm, suffer a more distal injury, and have their operation within 24 months of the injury. About 49% of the patients in this study experienced “good to excellent” recovery and were significantly more likely to exhibit the aforementioned characteristics. Sunderland made similar conclusions that earlier repairs have better outcomes, single function nerves recover more than multifunctional nerves, distal grafts do better than proximal ones, and that shorter graphs typically recover better than long ones.[8]
Proper technique in nerve grafting provides the best possible outcome for the patient. Blunt and sharp nerve ends with bundle-to-bundle matching before suturing the components of the cable graft result in more effective reinnervation.[6] It is also important to note that reversal of the orientation of the nerve graft provides a better outcome because more axons regenerate distally rather than scattering laterally through branches.[14] Approximating the diameter of the graft with the diameter of the injured nerve is another essential task. In this presented case, because the femoral nerve is considerably larger than the proposed autograft donor, the cable graft technique was used.[48] Creating grafts of different lengths allows proper reinnervation without tension placed between the two suture sites, which would promote avulsion and scarring around the graft connections.[8]
Based on this data, recovery of our patient's motor function can be attributed to his young age, brevity between the accident and the operation, the operative techniques used, and physical therapy with use as tolerated of the affected leg.[9] Although young age is a good prognostic indicator, we were unable to identify a successful cable graft procedure in a patient as young as ours at 21 months who had sustained a complete nerve transection. The shortest possible amount of time between the accident and the operation minimizes the time available for Wallerian degeneration and end-organ damage to occur, preventing endoneurial tube shrinking and fibrosis, and ensuring effective reinnervation of the quadriceps muscles by managing the femoral artery laceration and soft-tissue damage.[10]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Peripheral nerve reconstruction after injury: A review of clinical and experimental therapies. Biomed Res Int 2014 2014:698256.
- [Google Scholar]
- Chapter 8: Current techniques and concepts in peripheral nerve repair. Int Rev Neurobiol. 2009;87:141-72.
- [Google Scholar]
- Biomedical engineering strategies for peripheral nerve repair: Surgical applications, state of the art, and future challenges. Crit Rev Biomed Eng. 2011;39:81-124.
- [Google Scholar]
- The role of current techniques and concepts in peripheral nerve repair. Plast Surg Int 2016 2016:4175293.
- [Google Scholar]
- An analysis of the results of late reconstruction of 132 median nerves. J Hand Surg Br. 1993;18:97-105.
- [Google Scholar]
- Bunge memorial lecture. Nerve injury and repair – A challenge to the plastic brain. J Peripher Nerv Syst. 2003;8:209-26.
- [Google Scholar]




