
Translate this page into:
Nonadherence to Antiepileptic Medications: Still a Major Issue to be Addressed in the Management of Epilepsy
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
Medication nonadherence is a significant barrier in achieving seizure freedom in patients with epilepsy. There is a deficiency of data about the reasons for nonadherence in Saudi population.
Aims:
The aim of this study is to prove the existence of nonadherence to antiepileptic drugs (AEDs) in patients with epilepsy and identify the responsible factors.
Setting and Design:
This is a prospective, cross-sectional study carried in the Department of Neurology at King Fahd Hospital of the University affiliated with Imam Abdulrahman Bin Faisal University.
Subjects and Methods:
Patients of all ages diagnosed to have epilepsy as mentioned in their medical record and taking antiepileptic medications were interviewed using a questionnaire.
Statistical Analysis Used:
Statistical analysis was performed using IBM Statistical Package for the Social Sciences version 21 (IBM Corp., Armonk, NY, USA). Statistical significance was defined as two-tailed with a P ≤ 0.05.
Results:
Among 152 participants, 52.6% were male and 47.4% were female. Mean age of the patients was 28 ± 14.3 (mean ± standard deviation) years. Of 152 patients, 48.7% were found to be nonadherent to their AED therapy. The most commonly identified factor was forgetfulness. Nonadherence was significantly associated with poor seizure control (P = 0.002).
Conclusion:
Nonadherence to the AED is common among patients with epilepsy and affects seizure control adversely.
Keywords
Antiepileptic drugs
epilepsy
nonadherence

INTRODUCTION
Epilepsy is characterized by recurrent, unprovoked epileptic seizures and can affect people of all age groups. The overall estimated worldwide prevalence of epilepsy is 10/1000 population.[1] Approximately, 50 million people live with epilepsy all over the world, and nearly 75% belong to resource-poor countries with less accessibility to proper healthcare facilities.[2] The prevalence rate (PR) of active epilepsy in Saudi Arabia (SA) is 6.5/1000 population.[3] The management of epilepsy includes not only proper antiepileptic drug (AED) therapy but also identification of goals and development of proper care plan as well.[4] The ultimate goal is freedom from seizure along with improvement in the quality of life,[5] and this cannot be achieved if patient develops repeated seizures due to poor compliance to AED. Medication adherence has been defined as the extent to which a patient follows the instruction for a prescribed medication by a physician and persistence as the duration of time from initiation to discontinuation of treatment.[6] Nonadherence to medication is one of the most serious impediments in clinical practice,[7] and this phenomenon in patients with epilepsy can lead to loss of seizure control,[8] resulting in failure to achieve the treatment goal which can otherwise be expected in up to 70% of patients with optimal AED therapy.[9] The measurement of patient's adherence to medications and use of interventions to improve it are not being practiced routinely.[10] Medication nonadherence rate among patients with epilepsy ranges from 30% to 60%.[11] As a consequence of AED nonadherence, patients can have serious consequences such as increased risk of status epilepticus[12] and sudden unexplained death in epilepsy patients.[13] A recent systematic review observed a PR of AED nonadherence ranging from 29% to 66% and suggested that a comprehensive adherence assessment should be a routine practice.[14] In a study from SA assessing the medication adherence among patients with epilepsy, 38.3% were found to be nonadherent to their treatment.[15] Frequency of administration, difficulty in swallowing, and side effects are the major medication-related factors responsible for nonadherence along with inability of a patient to understand the importance of taking medications and fear of getting stigmatized in the society by their diagnosis.[16] Accurate measurement of adherence is difficult. Self-reporting, monitoring of drug levels, and monitoring of prescription refilling are some methods to measure adherence.[8] Adherence can be overestimated if measured by self-reporting due to self-presentation bias.[17] Medications adherence may be affected by cultural or psychosocial factors as well.[18] Every country and society has different culture and trends. One study addressing the awareness of epilepsy and its management in Riyadh, SA, found that only 49% of respondents had belief in the importance of seeking medical advice while remaining believed in faith, spiritual treatment, and herbal medication. The authors concluded that there is a need to improve awareness about epilepsy in Saudi population.[19] There is a paucity of data regarding the issue of nonadherence and responsible factors from our region. This study was aimed to identify the extent of nonadherence in patients with epilepsy and determine the responsible factors.
SUBJECTS AND METHODS
This is a prospective, cross-sectional study carried out in the Department of Neurology at King Fahd Hospital of the University over the duration of 1 year starting from August 2016 till the end of July 2017 after getting approval by the institutional ethical committee of the university. We recruited patients from epilepsy clinic. The Department of Neurology has a separate specialized epilepsy clinic headed by a qualified epileptologist. Patients of all ages diagnosed to have epilepsy as mentioned in their medical record and taking AED therapy were included. Patients who were seizure free for >3 years and diagnosed to have epilepsy within 6 months were excluded from the study. A minimum sample size of 141 patients was calculated using the Daniel 1999 based formula for finite population, assuming an estimated adherence to AED as 50%,[11] precision of 6% (0.06), and an available population of 300 patients with 95% confidence limits. The data were collected using a questionnaire after taking written consent from the patient and/or guardian (caregiver). Patients and caregivers were assured of maintaining the privacy and confidentiality of their personal information. The questionnaire was explained in detail to the physicians involved in data collection. The questionnaire comprised questions regarding demographic characteristics (age, gender, and occupation), information about level of dependency, age at the time of diagnosis, duration of disease, family history of epilepsy, type and frequency of seizures, and current antiepileptic medications. Seizure was classified as primary generalized, secondary generalized, simple partial, complex partial, and unclassified. Frequency of seizure was also documented as seizure free >2 years, seizure free >1 year, seizure 6 months ago, and seizure almost every 2–3 months, every month, and every week. Unsure term was used for those who were not sure about their frequency of seizures. Those who were seizure free for at least 6 months or more were defined as having well-controlled seizures. Patients who had seizures in previous 6 months were labeled as having poorly controlled seizures. Findings of relevant investigations as electroencephalogram (EEG) and brain imaging either computerized tomography or magnetic resonance imaging were noted. EEG findings were described as normal, diffuse neuronal dysfunction, and epileptiform discharges (EDs). EDs were classified as focal, generalized, multifocal, and focal as well as generalized. Details about AED therapy as number of medications, generic name, and serum drug levels where applicable were also entered. Adherence to medications was measured by asking patients whether they ever missed or stop their medications. Patients who did not miss or stop their medications were considered adherent as described in a study from China.[20] When nonadherence was recognized, further questions related to understanding about the disease, medications, counseling by treating physicians’ and patients’ related factors such as pregnancy and breastfeeding among female patients were also asked to identify the possible responsible factor.
Statistical analysis was performed using IBM Statistical Package for the Social Sciences version 21 (IBM Corp., Armonk, NY, USA). Descriptive statistics were analyzed as frequency and percentages for qualitative variables. The mean values ± standard deviation (mean [SD]) was used for quantitative variables. Pearson's Chi-square test was used to find association between AED therapy adherence and nominal independent variables. We used the Chi-squared test, t-test, and Pearson's correlation when appropriate. Statistical significance was defined as two-tailed with a P ≤ 0.05.
RESULTS
This prospective, cross-sectional study included 168 patients who met the inclusion criteria, and 152 patients agreed to participate and completed the questionnaire. Among 152 patients, 80 (52.6%) were male and 72 (47.4%) female with no significant difference in gender distribution. Mean age of the patients was 27.9 (14.3) (mean [SD]) years. Out of 152 patients, 74 (48.7%) were nonadherent and 78 (51.3%) were adherent to their AED therapy. Majority of the patients were between 11 and 40 years of age, and most of them were diagnosed to have epilepsy between 1 and 10 years. Regarding occupational status, 30% were students, 20% staying at home, 17% homemakers, 8% professionals, and 6% were involved in office work. Family history of epilepsy was found in 22% of patients only. Secondarily, generalized seizure was the most common seizure type, identified in 49% of patients. Patient's demographic characteristics and other relevant details in both groups of patients are summarized in Table 1.
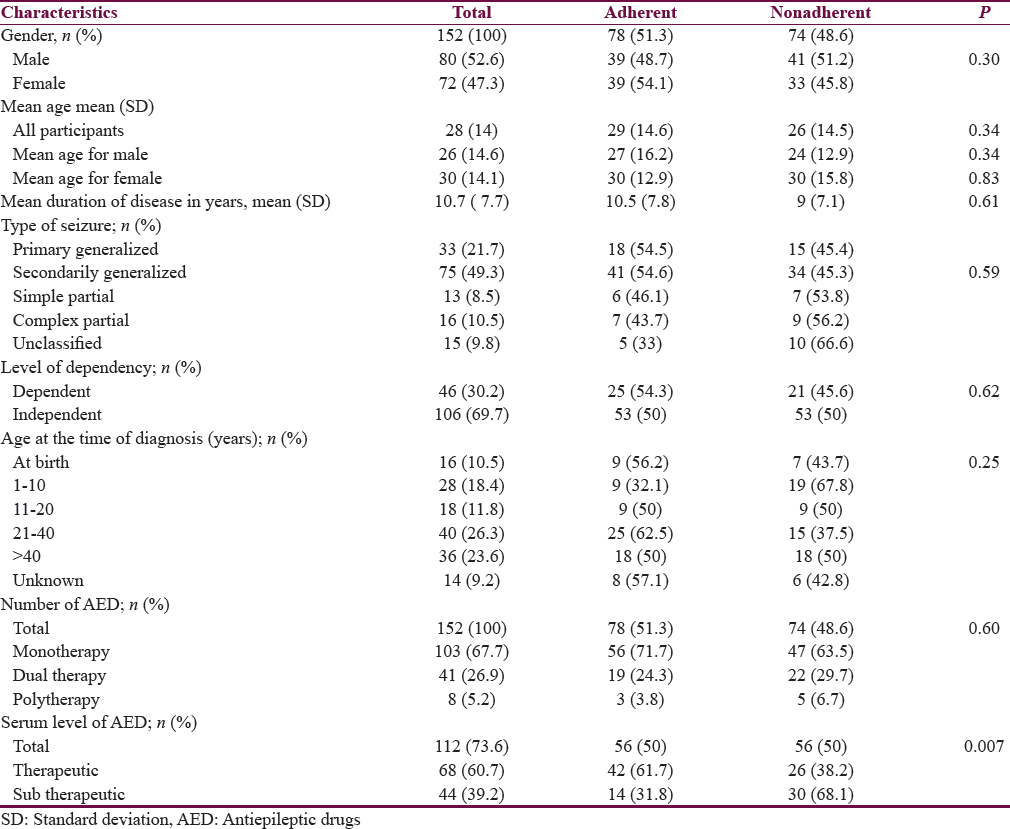
The most commonly identified abnormal finding on EEG was focal interictal epileptic discharges (IEDs), reported in 30% of recordings. Generalized IEDs reported in 17% and focal as well as generalized in 4%. Diffuse slowing of background rhythm suggestive of diffuse neuronal dysfunction was reported in 9% of recordings. Among all epileptic patients, 103 were on monotherapy, 41 on dual therapy, and 8 on polytherapy. Carbamazepine was the most commonly prescribed AED (47%), followed by valproic acid (34%), levetiracetam (26%), and phenytoin (10%). Other prescribed medications were lamotrigine (10%), topiramate (6.2%), and clonazepam (5%). Phenobarbitone was taken by only 1.4% of patients. Monitoring of serum level of AED was recommended in 137 patients and was available for 112 patients. Significantly higher number of patients in nonadherent group was found to have subtherapeutic levels compared with adherent group (P = 0.00).
The common factors leading to nonadherence are shown in Figure 1. The most commonly identified factor was forgetfulness to take the medication followed by lack of time due to busy schedule. Regarding seizure control, nonadherence was significantly associated with poor seizure control (P = 0.00) as shown in Figure 2. Exact frequency of seizure was obtained in 146 (96%) participants. 71 (48.6%) patients were found to have poor seizure control and 75 (51.3%) patients had well-controlled seizures. Among patients with poorly controlled seizures, significantly greater number of patients nonadherent to their medication was found to have increased frequency of seizures compared with patients who were adherent to their medications (P = 0.00) as shown in Figure 3.

- Common factors responsible for nonadherence to antiepileptic medications

- Number of patients with well-controlled and poorly controlled seizures in both groups

- Frequency of seizures in compliant and noncompliant patients
DISCUSSION
Nonadherence to AED therapy has been considered as a major hindrance in achieving therapeutic goal is freedom from the seizures in epileptic patients. In our study, nonadherence was identified in 48.7% of patients. It was higher than reported in a recent hospital-based study from Riyadh, SA, by Gabr and Shams.[15] In their study, nonadherence was found in 38.3% of the participants.[15] In a community-based study on epilepsy by Buck et al., 72% of patients were found to be compliant, while 28% accepted that they missed their AED.[21] In another study, recruiting 54 patients from hospital epilepsy clinic, 32 (59%) patients were classified as nonadherent to their medications.[8] The prevalence of nonadherence to AED therapy was reported as high as 64% in a clinic-based study from Malaysia[22] and 66.2% from Brazil.[23] Nonadherence rate comparable with our study was reported by Liu et al. (48.1%)[20] and Molugulu et al. (49.3%).[24] The difference may be explained by different selection criteria and use of different instruments to measure adherence and cultural behaviors of participants. People living in different countries have difference in their cultures and social values and hence can have variation in their behavior toward therapy. In a study from SA, Alaqeel and Sabbagh have revealed that 16.2% of participants considered epilepsy as being untreatable and around 50% believed in nonmedical treatment.[19] This study was followed by awareness campaign. Similar campaigns should be organized to increase the level of awareness about AED as well.
We could not find any statistically significant association of demographic features such as age and gender with AED adherence. This finding is similar to other studies describing the factors related to adherence with AEDs.[82223] Significant association between age and self-reported adherence has been observed by other researchers.[2122] Buck et al. reported that failure to comply is more common in younger patients,[21] and Tan et al.[22] found that 74.2% of the patients with poor adherence were below 40 years of age. One study has reported a 3% reduction in AED nonadherence probability with 1 year increment in age.[23] In our study, no association was found between gender and adherence rate and this finding is similar to other studies.[152025] In contrast to our study, other researchers have found women more likely to be adherent to AEDs as compared with men.[232627] Further large sample-sized studies are warranted to show the exact relationship of age and gender with medication nonadherence from our region.
The age of onset and duration of disease can also have an effect on adherence rate of medications. Longer duration of disease is considered to have an adverse effect on compliance.[2829] In another study, the omission of dose was found more frequent with longer duration of treatment.[7] Liu et al. found the longer duration of treatment as the only factor that affected the AED adherence.[20] In contrast to these studies, a significant positive correlation was shown between duration of epilepsy and adherence by Tan et al.[22] It was postulated that patients with longer disease duration perceive taking their AEDs as part of routine life. However, no association was found between the duration of disease and adherence to AEDs in our study and this finding is in agreement with other studies including one study from SA.[152326] No significant association could be made between the rate of nonadherence and seizure type. Ferrari et al. and Guo et al. also could not correlate the rate of nonadherence to specific epilepsy syndrome and seizure type, respectively.[2326] No significant difference in AED adherence was found in patients with generalized compared with patients having focal epilepsy by Gabr and Shams, as well.[15] In our study, AED adherence did not differ significantly in patients on monotherapy from patients on dual and polytherapy. Although nonadherence rate was relatively higher in patients on polytherapy and dual therapy compared with monotherapy, it was statistically insignificant (P = 0.62) as detailed in Table 1. Nonadherence was not found to be associated with mono or polytherapy/number of medications by Guo et al. and Sweileh et al. as well.[2630] On the other hand, some investigators have found that patients on monotherapy were significantly more adherent than patients on polytherapy.[1523] Seizure frequency and control were significantly associated with adherence rate (P = 0.00) in our study, and this finding is similar to published literature. Patients who were not adherent to their medications were found to have poor seizure control as compared with patients who were adherent to their AEDs. Other studies have also proven significant association between frequency of seizure and nonadherence rate.[152326] Poor seizure control was found to be significantly associated with nonadherence by Jones et al. and Hovinga et al. as well.[831] Forgetfulness was the most common factor followed by lack of time due to busy daily schedule, leading to nonadherence in our cohort of patients; similar observation was reported by Ferrari et al.[23] Forgetfulness has been reported as the primary reason for nonadherence by Gabr and Shams (50%),[15] Liu et al. (69.9%),[20] and Hovinga et al. (72%)[31] as well. Polytherapy, side effects of medication, and inadequate counseling by the treating physician were reasons for nonadherence in nearly equal number of patients. The reported prevalence of nonadherence to AED and identified factors/predictors influencing the compliance in different studies are summarized in Table 2.

The limitation of our study is its relatively smaller sample size and convenient sampling. Patients were recruited only from the clinic of our hospital, and this limits the implication of results being generalized. Some patients were dependent on their caregivers for medications. Factors such as educational status, depression, anxiety, and quality of life were not assessed. Cost of medication and financial status of patients which are reasons for nonadherence in some countries were not studied as this study is from government hospital and patients do not pay for medications. Adherence may be affected in month of Holy Ramadan as most of the Muslim patients practice fast and this should be studied as well. There is a real need to carry out further studies incorporating validated questionnaires to assess the prevalence of nonadherence to AED accurately and addressing factors which might affect adherence significantly and were not studied in the current study as socioeconomic and educational status, personal beliefs about illness and medications, and level of care provided by caregiver in patients who are dependent.
CONCLUSION
This hospital-based study from Eastern Province of Kingdom of SA reveals that nonadherence to AED is common among patients with epilepsy and affects seizure control adversely. Association of AED nonadherence with demographic features such as age, gender, and occupational status needs to be further studied by large sample size studies. Forgetfulness is the primary reason for nonadherence and can be improved by making diaries, digital reminders, and alarms. Treating physicians should counsel in detail about the impact of AED nonadherence on seizure control to the patients. Strategies should be implemented to assess adherence comprehensively as part of routine clinical practice which can otherwise be a reason for apparent treatment failure. Awareness campaigns should be organized in community at institutional and national level to increase the awareness.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
This research made use of the computational resources and technical services provided by the Scientific and High-Performance Computing Center at Imam Abdulrahman Bin Faisal University.
REFERENCES
- Prevalence and pattern of epilepsy treatment in different socioeconomic classes in Brazil. Epilepsia. 2007;48:880-5.
- [Google Scholar]
- Estimation of the burden of active and life-time epilepsy: A meta-analytic approach. Epilepsia. 2010;51:883-90.
- [Google Scholar]
- The prevalence of epilepsy and other seizure disorders in an Arab population: A community-based study. Seizure. 2001;10:410-4.
- [Google Scholar]
- A study on drug use evaluation of antiepileptics at a multispecialty tertiary care teaching hospital. Int J Pharm Tech Res. 2009;1:1541-7.
- [Google Scholar]
- Antiepileptic drugs and cognitive impairment in epileptic patients at a private hospital. Res J Pharm Biol Chem Sci. 2011;2:824-9.
- [Google Scholar]
- Measuring the rate of therapeutic adherence among outpatients with T2DM in Egypt. Saudi Pharm J. 2010;18:225-32.
- [Google Scholar]
- The relationship between poor medication compliance and seizures. Epilepsy Behav. 2002;3:338-42.
- [Google Scholar]
- Adherence to treatment in patients with epilepsy: Associations with seizure control and illness beliefs. Seizure. 2006;15:504-8.
- [Google Scholar]
- Managing patient adherence and quality of life in epilepsy. Neuropsychiatr Dis Treat. 2007;3:117-31.
- [Google Scholar]
- Medication adherence: Its importance in cardiovascular outcomes. Circulation. 2009;119:3028-35.
- [Google Scholar]
- Prevalence and cost of nonadherence with antiepileptic drugs in an adult managed care population. Epilepsia. 2008;49:446-54.
- [Google Scholar]
- Adult convulsive status epilepticus in the developing country of honduras. Seizure. 2010;19:363-7.
- [Google Scholar]
- Forensic antiepileptic drug levels in autopsy cases of epilepsy. Epilepsy Behav. 2011;22:778-85.
- [Google Scholar]
- Identifying the barriers to antiepileptic drug adherence among adults with epilepsy. Seizure. 2017;45:160-8.
- [Google Scholar]
- Adherence to medication among outpatient adolescents with epilepsy. Saudi Pharm J. 2015;23:33-40.
- [Google Scholar]
- A Question of Choice Compliance in Medicine Taking. A Preliminary Review (2nd ed). London: Medicine Partnership; 2003.
- Patient self-reporting of compliance does not correspond with electronic monitoring: An evaluation using isosorbide dinitrate as a model drug. Pharmacotherapy. 1997;17:126-32.
- [Google Scholar]
- Racial and ethnic differences in response to medicines: Towards individualized pharmaceutical treatment. J Natl Med Assoc. 2002;94:1-26.
- [Google Scholar]
- Adherence to treatment and influencing factors in a sample of Chinese epilepsy patients. Epileptic Disord. 2013;15:289-94.
- [Google Scholar]
- Factors influencing compliance with antiepileptic drug regimes. Seizure. 1997;6:87-93.
- [Google Scholar]
- Factors influencing adherence to antiepileptic drugs therapy in Malaysia. Neurol Asia. 2015;20:235-41.
- [Google Scholar]
- Factors associated with treatment non-adherence in patients with epilepsy in Brazil. Seizure. 2013;22:384-9.
- [Google Scholar]
- Evaluation of self-reported medication adherence and its associated factors among epilepsy patients in hospital Kuala Lumpur. J Basic Clin Pharm. 2016;7:105-9.
- [Google Scholar]
- Evaluation of factors influencing medication adherence in patients with epilepsy in rural communities Kaduana State Nigeria. Neurosc Med. 2011;2:299-305.
- [Google Scholar]
- Depression and anxiety are associated with reduced antiepileptic drug adherence in Chinese patients. Epilepsy Behav. 2015;50:91-5.
- [Google Scholar]
- Adherence to medicines and self-management of epilepsy: A community-based study. Epilepsy Behav. 2013;26:109-13.
- [Google Scholar]
- Noncompliance with immunnosuppressive medications after renal transplantation. Exp Clin Transplant. 2003;1:39-47.
- [Google Scholar]
- Is tolerance induction the answer to adolescent non-adherence? Pediatr Transplant. 2005;9:357-63.
- [Google Scholar]
- Self-reported medication adherence and treatment satisfaction in patients with epilepsy. Epilepsy Behav. 2011;21:301-5.
- [Google Scholar]
- Association of non-adherence to antiepileptic drugs and seizures, quality of life, and productivity: Survey of patients with epilepsy and physicians. Epilepsy Behav. 2008;13:316-22.
- [Google Scholar]




