
Translate this page into:
Isolated Wrist Drop Presenting as Acute Stroke: Rare Case Report with Review of Literature
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Isolated wrist drop is very unusual clinical presentation due to cerebral stroke. It is highly confused with peripheral neuropathy. However, timely detection of acute stroke as one of the causes of wrist drop is necessary as it changes the line of treatment and prognosis significantly. Here we are presenting a 62 year-old diabetic and hypertensive male patient who came with acute onset weakness of right hand. Initial Magnetic resonance imaging (MRI) of the brain showed hyperacute infarct in the splenium of corpus callosum. Magnetic resonance angiography (MRA) was normal. Repeat brain MRI on next day showed acute infarct at hand area of motor strip in posterior frontal region. The patient underwent intravenous thrombolysis and thereafter improved significantly. Isolated hand palsy is a rare presentation of stroke, often mistaken for peripheral lesion.
Keywords
Isolated wrist drop
posterior frontal
splenium
thrombolysis

INTRODUCTION
Isolated wrist drop is usually considered due to peripheral nerve lesions. Rarely, it is a presentation of acute stroke, in which case an early and prompt diagnosis is important to initiate the timely treatment to prevent permanent deficits and further progression of the disease. It is important to differentiate the cause as management of wrist drop due to stroke is different than due to peripheral pathology. We report a case of acute ischemic stroke who presented with isolated wrist drop which was managed aggressively with improved outcome. Furthermore, we are reviewing the literature on this peculiar presentation of acute stroke.
CASE REPORT
A 62-year-old gentleman presented with sudden onset of numbness in the right hand followed by inability to lift fingers along with wrist for the half an hour. On examination, the patient was alert, oriented with normal speech, without cranial nerve deficits. Power was full in all four limbs except in the right wrist and fingers where it was Grade 1. Sensory examination including cerebellar system examination was normal. There were no sensory deficits at the right wrist and fingers also. He was having a history of left-sided weakness 10 years ago which improved completely. He was diabetic and hypertensive. Routine and special blood investigations with coagulation profile were normal. Thyroid functions and serum vitamin levels of B12 and folic acid were also normal. Initial diagnosis of radial neuropathy was ruled out by nerve conduction studies and electromyography. Brain magnetic resonance imaging (MRI) and magnetic resonance angiography revealed acute infarct in the splenium of corpus callosum, with no evidence of major intracranial arterial occlusion and normal rest of the brain parenchyma [Figure 1a and b]. Repeat brain MRI was done the next day. It showed acute infarct at the hand region of motor area in the posterior frontal lobe [Figure 1c and d]. The patient was thrombolyzed with intravenous tissue plasminogen activator (tPA). Postthrombolysis, the patient had considerable symptomatic improvement which was maintained till the time of discharge.
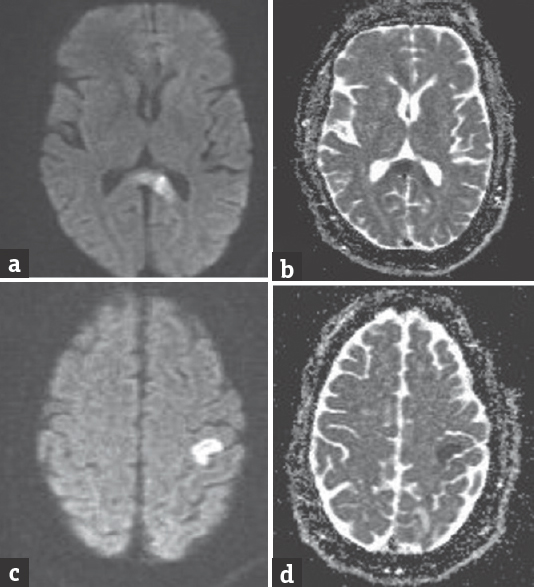
- (a and b) Diffusion-weighted imaging and apparent diffusion coefficient of the first magnetic resonance imaging brain showing splenial infarct. (c and d) Diffusion-weighted imaging and apparent diffusion coefficient of the second magnetic resonance imaging brain showing infarct at the left precentral gyrus
DISCUSSION
Isolated hand weakness (drop hand) develops either from a central cause or from a peripheral cause. On presentation, we suspected it as a peripheral lesion of radial nerve. However, sensory symptoms were absent. Nerve conduction studies were normal. As the patient was at higher risk for stroke, it was considered as one of the diagnoses and evaluations done.[1] Embolic stroke of the hand knob area or small lacunar infarct is considered as one of the causes for unilateral wrist drop.[1] It has been reported by Kim that ulnar-like deficits are associated with severe stenosis or occlusion of the carotid artery, whereas radial-like deficits are associated with an embolic mechanism.[2] Our patient was not having any significant primary diagnosis, but it was presumed to be silent emboli stroke. The patient was having risk factors such as old age, diabetes, and hypertension with previous history of vascular events.
After suspecting stroke, brain MRI was done. First MRI was showing splenial infarct, which did not explain hand weakness. However, there are case reports of radial-like deficits in the hand with different localizations in the brain. A case of the right wrist drop with lesion in the middle and posterior cerebral arteries (MCAs and PCAs) watershed territory has been reported previously.[3] Another case of wrist drop following an anterior cerebral artery (ACA) and MCA border zone infarct has been also described.[3] However, splenial infarct was not explaining this weakness. Hence, MRI was repeated which revealed left precentral gyrus hand area infarct. Intravenous tPA was given, and the patient recovered significantly.
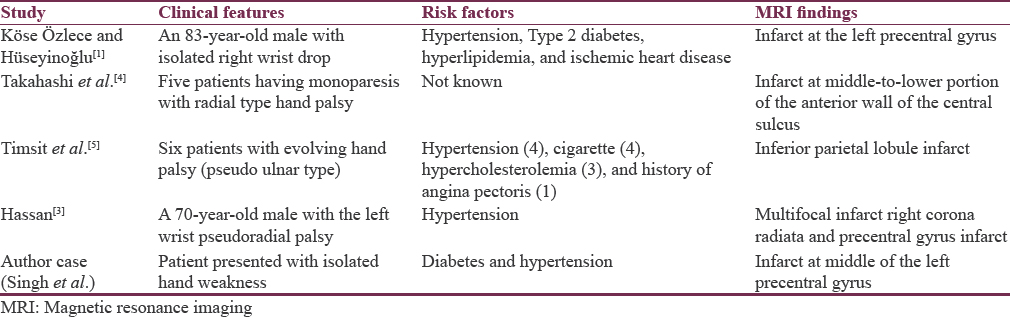
Takahashi et al. recognized isolated radial type hand palsy in five patients and localized it at infarct of middle-to-lower portion of the anterior wall of the central sulcus.[4] According to Timsit et al., six patients presented with pseudoulnar type evolving palsy of the hand. Each was having one or other risk factors for carotid stenosis such as hypertension, hypercholesterolemia, cigarette smoking, and history of angina. Infarction was localized at the junction of ACA, MCA, and PCA at inferior parietal lobule.[5]
Finally, to diagnose isolated hand drop as an acute motor area stroke is very difficult. However, high-risk factors such as old age, diabetes, and hypertension should confirm your diagnosis in case of normal nerve conduction studies as happened in our case. High degree of clinical suspicion should be maintained so that such salvageable disorder should not be missed out. Table 1 was showing similar case reports by various authors comparing to our case.
CONCLUSION
Isolated unilateral wrist drop is often misdiagnosed as peripheral nerve palsies. It is important to keep differential diagnosis of acute stroke in mind to rule out causes for isolated hand weakness as early aggressive treatment can prevent permanent deficits. Advance sequences such as diffusion sequence MRI are very helpful in the early diagnosis of stroke.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- A rare clinical presentation due to small cortical infarction: Isolated wrist drop. Turk J Cerebrovasc Dis. 2015;21:36-9.
- [Google Scholar]
- Predominant involvement of a particular group of fingers due to small, cortical infarction. Neurology. 2001;56:1677-82.
- [Google Scholar]
- Fractional arm weakness as presentation of stroke due to posterior borderzone infarct: A report of two cases. Ann Indian Acad Neurol. 2010;13:302-4.
- [Google Scholar]
- Isolated hand palsy due to cortical infarction: Localization of the motor hand area. Neurology. 2002;58:1412-4.
- [Google Scholar]
- Evolving isolated hand palsy: A parietal lobe syndrome associated with carotid artery disease. Brain. 1997;120(Pt 12):2251-7.
- [Google Scholar]




