
Translate this page into:
Brachial branches of the medial antebrachial cutaneous nerve: A case report with its clinical significance and a short review of the literature
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The medial antebrachial cutaneous nerve (MACN) is a branch of the brachial plexus with a great variation within its branches. Knowledge of these variations is critical to neurologists, hand surgeons, plastic surgeons, and vascular surgeons. The aim of this study was to search for variations of the MACN and to discuss their clinical significance. For this study, six arm cadavers from three fresh cadavers were dissected and examined to find and study possible anatomical variations of the MACN. The authors report a rare case of a variation of the MACN, in which there are four brachial cutaneous branches, before the separation to anterior (volar) and posterior (ulnar) branch, that provide sensory innervation to the medial, inferior half of the arm, in the area that is commonly innervated from the medial brachial cutaneous nerve. To our knowledge, this is the first documented case of this nerve variation. This variation should be taken into serious consideration for the differential diagnosis of patients with complaints of hypoesthesia, pain, and paresthesia and for the surgical operations in the medial part of the arm.
Keywords
Anatomical variations
clinical anatomy
medial antebrachial cutaneous nerve
medial cutaneous nerve of the forearm

Introduction
The medial antebrachial cutaneous nerve (MACN) arises from the medial cord of the brachial plexus and is derived from segments C8 and T1.[12] It courses on the upper arm, pierces the brachial fascia with the basilic vein, about 10 cm above the medial epicondyle, and emerges most commonly as two branches, the anterior and the posterior, which continue downward as far as the wrist.[134] Its function is to provide sensory innervation to the skin of the medial forearm and the skin over the olecranon.[5]
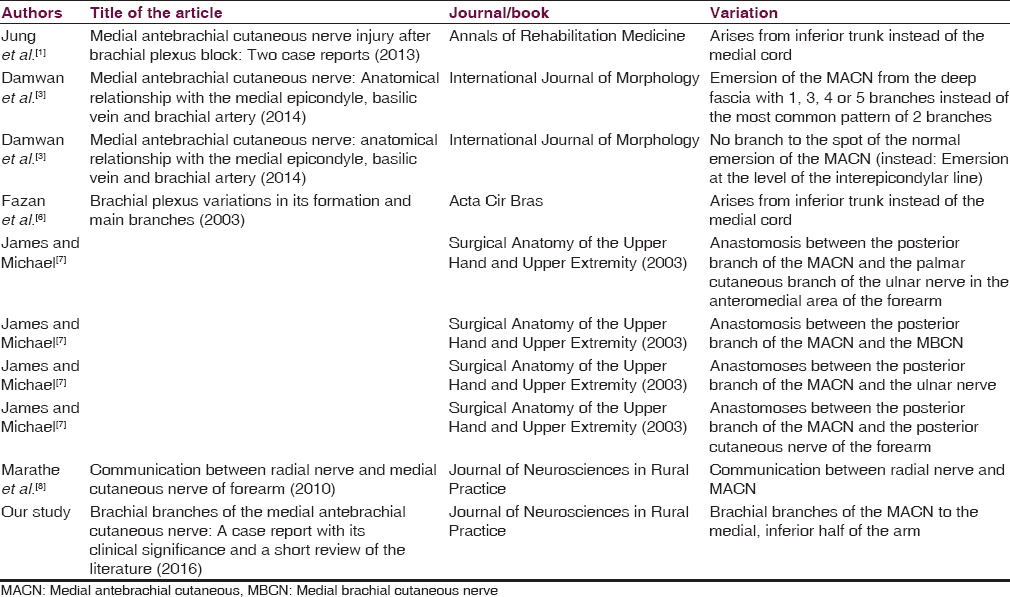
The MACN is related to a great amount of variations [Table 1]. The authors report a variation in which the MACN provides four branches to the medial, inferior half of the arm. Although the cases in the literature describing variations of the branches of the brachial plexus are abundant, there is not any similar case describing brachial branches of the MACN in this specific area.[26] The presence of this anatomic variation can be used to explain unexpected clinical, neurological signs and symptoms, such as hypoesthesia or dysesthesia in the area of the arm.[6]
Case Report
Six fresh cadaveric arms were dissected. All the three cadavers were in the anatomical position with the forearms supinated. After removing the skin and revealing the subcutaneous tissue, the MACN was isolated from the adipose tissue and examined. In addition, the brachial fascia was removed to study the brachial course of the nerve from its origin, the brachial plexus, to its emersion from the brachial fascia. Five of six nerves had no significant variations. One of them, the one of the female cadaver was providing branches to the skin of the medial, inferior half of the arm, in the area that is commonly innervated by the medial brachial cutaneous nerve (MBCN). The authors isolated the nerve from the basilic vein and examined the number, the thickness, the length, and the allocation of the brachial cutaneous branches. There were four branches, about 1.0–2.0 mm in diameter and 4.3–10.5 cm in length, in the area of the medial, inferior half of the arm [Figures 1 and 2]. The most superior branch was separated from the MACN 14.2 cm above the medial epicondyle, the second one 12.4 cm, the third one 7.6 cm, and the most inferior one 5.6 cm above the medial epicondyle. Measurements were made by using a meter.

- Brachial course of the right medial antebrachial cutaneous nerve of a female cadaver. 1-4: Brachial branches of the medial antebrachial cutaneous nerve, BB: Biceps brachialis, BV: Basilic vein, MACN: Medial antebrachial cutaneous nerve, MN: Median nerve, UN: Ulnar nerve

- Brachial course and separation into anterior and posterior branch of the right medial antebrachial cutaneous nerve of a female cadaver. 1-4: Brachial branches of the medial antebrachial cutaneous nerve, BB: Biceps brachialis, CV: Cephalic vein, BV: Basilic vein, MACN: Medial antebrachial cutaneous nerve, MN: Median nerve, UN: Ulnar nerve, AbMACN: Anterior branch of medial antebrachial cutaneous nerve, PbMACN: Posterior branch of medial antebrachial cutaneous nerve
Discussion
The brachial plexus is a network of nerves that is formed by the anterior rami of the lower four cervical nerves and first thoracic nerve (C5–C8, T1). It is divided into five roots, three trunks, six divisions, and three cords and innervates the upper limb.[2] To be more specific, the MACN originates from the medial cord and is derived from segments C8 and T1. At the area of the arm, it courses distally with the median nerve, the ulnar nerve, the brachial artery, and the basilic vein until it pierces the deep fascia 10 cm above the medial epicondyle where it emerges as two branches, the anterior (volar) and the posterior (ulnar) branch.[34] Its function is to provide sensory innervation in the medial forearm and the skin over the olecranon.[5]
The literature includes an amount of variations of the MACN [Table 1]. Knowledge of nerve variations in anatomy is of high significance for anatomists, neurologists, and surgeons. In our study, we found an unusual variation of the MACN in which the MACN provides sensory innervation to the medial, inferior half of the arm. The variation was not bilateral but existed only on the right arm. That probably means that the percentage of appearance may be lower than we expect it to be. We have to study this variation on a bigger population to have a reliable result.
This study has not only anatomical significance but also clinical. Paresthesia, numbness, dysesthesia, and acute pain are the neurological problems mentioned in the literature when an MACN injury exists.[19] Injury to MACN could happen to the nerve itself, to its branches, to the medial cord, or to segments C8 to T1. All ways could cause the neurological symptoms mentioned above.[1] The literature states that MACN neuropathy causes neurological disorders on the medial forearm and the anteromedial aspect of the elbow.[19] In the case of our study, a possible injury to the MACN would also cause numbness, pain, and other disorders in the medial, inferior half of the arm, in a specific area that is innervated from the MBCN.[2] An unaware neurologist that does not have this case in his/her mind would suppose that injury in the MBCN also exists except from the MACN injury. The differential diagnosis can become difficult because according to the literature, electrophysiological examination of MACN nerve is not an everyday upper extremity electrodiagnostic examination and that explains why some MACN injuries may remain undiagnosed.[1]
Even though it is rarely reported, MACN injury associated with iatrogenic etiologies is possible.[1] The possible causes are local anesthesia, injuries by injection needles during brachial plexus block procedures, tumor, and routine venipuncture. Phlebotomy and cubital tunnel surgery has also been reported as an etiology.[910] The MACN might also been harmed during nerve repair operations, as the branches of the MACN are used as the “cable graft” for peripheral nerve repair. Damaging of the volar branch might cause mild (or none), often temporary, sensory, neurological problems.[11] The most frequent symptoms are dysesthisia, numbness, pain in the medial forearm, and painful paresthesia.[112] Things become more complicated if the MACN provides branches in the area of the medial arm, as the MBCN provides branches at the same area at about 15.3 cm proximal to the medial epicondyle.[13] To avoid inevitable confusion, hand surgeons and neurologists should have this case in their minds.
This case could also be interesting for plastic surgeons who undertake arm operations in the medial part of the arm. A good example could be brachioplasty because the traditional brachioplasty procedure involves incision running from the medial epicondyle to the axilla.[13] It is very important to avoid injuring the MBCN in the medial arm and the interocostobrachial nerve in the axilla.[14] Brachial branches from the MACN could raise the possibilities of nerve injuries and appearance of neurological problems as the branches in the surgical area would be more in amount.
Medical-surgical specializations that are not directly related to the nerves, such as vascular surgeons, may also find useful and necessary the knowledge of the MACN variations. In case of vascular surgery, peripheral nerves can be damaged during vascular access operations, and this fact causes neurological dysfunctions. A new method, in which axial splitting of MACN branches takes place, facilitating second-stage elevation of basilic and brachial vein in patients with arteriovenous fistula, was described.[15]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Medial antebrachial cutaneous nerve injury after brachial plexus block: Two case reports. Ann Rehabil Med. 2013;37:913-8.
- [Google Scholar]
- Variations in brachial plexus and the relationship of median nerve with the axillary artery: A case report. J Brachial Plex Peripher Nerve Inj. 2007;2:21.
- [Google Scholar]
- Medial antebrachial cutaneous nerve: Anatomical relationship with the medial epicondyle, basilic vein and brachial artery. Int J Morphol. 2014;32:481-7.
- [Google Scholar]
- Determination of an ideal stimulation site of the medial antebrachial cutaneous nerve using ultrasound and investigation of the efficiency. Ann Rehabil Med. 2014;38:836-42.
- [Google Scholar]
- Anatomic course of the medial cutaneous nerves of the arm. J Hand Surg Am. 1991;16:48-52.
- [Google Scholar]
- Brachial plexus variations in its formation and main branches. Acta Cir Bras. 2003;18:14-8.
- [Google Scholar]
- Surgical Anatomy of the Upper Hand and Upper Extremity. Philadelphia: Lippincott Williams and Wilkins; 2003. p. :224.
- Communication between radial nerve and medial cutaneous nerve of forearm. J Neurosci Rural Pract. 2010;1:49-50.
- [Google Scholar]
- Paresthesia and forearm pain after phlebotomy due to medial antebrachial cutaneous nerve injury. J Brachial Plex Peripher Nerve Inj. 2011;6:5.
- [Google Scholar]
- Surgical treatment of painful neuroma in medial antebrachial cutaneous nerve. Ann Plast Surg. 2002;48:154-8.
- [Google Scholar]
- Use of the anterior branch of the medial antebrachial cutaneous nerve as a graft for the repair of defects of the digital nerve. J Bone Joint Surg Am. 1989;71:563-7.
- [Google Scholar]
- A rare cause of forearm pain: Anterior branch of the medial antebrachial cutaneous nerve injury: A case report. J Brachial Plex Peripher Nerve Inj. 2008;3:10.
- [Google Scholar]
- Avoiding the medial brachial cutaneous nerve in brachioplasty: An anatomical study. Eplasty. 2010;10:e16.
- [Google Scholar]
- Upper arm contouring with brachioplasty after massive weight loss. Arch Plast Surg. 2014;41:271-6.
- [Google Scholar]
- Axial splitting of the medial antebrachial cutaneous nerve facilitates second-stage elevation of basilic or brachial vein in patients with arteriovenous fistula. J Vasc Surg. 2015;62:1353-6.
- [Google Scholar]




