
Translate this page into:
A visit to the stroke belt of the United States
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Southeastern part of United States has been called the Stroke Belt due to a much higher incidence of stroke compared to the rest of the country. In this article, I summarize my 2 weeks of observations as a clinical preceptor at the Comprehensive Stroke Center, University of Alabama Hospital, Birmingham, AL. 57 patients were admitted during these 2 weeks, 61% had ischemic strokes, and 23% received intravenous recombinant tissue plasminogen activator (IV rt-PA). Endovascular neuro-interventionalists were performing diagnostic catheter angiography in 14% and emergent revascularization procedures in 7% of consecutive patients. Also, the stroke team enrolled 6 patients into National institute of health (NIH) funded clinical trials (3 Argatroban tPA stroke study (ARTSS), 2 Safety study of external counter pulsation as a treatment for acute ischemic stroke (CUFFS), 1 stenting and aggressive medical management for preventing recurrent stroke in intracranial stenosis (SAMMPRIS). In my opinion, these observations provided me with useful knowledge how to develop a cutting edge, proactive stroke treatment system. In particular, availability 24 × 7 and consistent application of a curative, “finding reasons to treat approach” coupled with state-of the-art technologies and skilled operators could make a huge difference.
Keywords
Cerebrovascular ultrasonography
stroke
thrombolysis

Introduction
The National Heart, Lung, and Blood Institute (NHLBI) has defined the Stroke Belt as those states that had a 1980 age-adjusted stroke mortality rate more than 10% above the average national rate. The Stroke Belt includes Alabama, Arkansas, Georgia, Indiana, Kentucky, Louisiana, Mississippi, North and South Carolina, Tennessee, and Virginia.[1] Recent studies further indicate that these regional and geographical differences are real with those being born in the Stroke Belt being twice likely to have a stroke than those born elsewhere in the US.[2] My interest in this region is further fostered by the need to understand the incidence and treatment needs of stroke patients in my native country, and the development of a stroke care system at my hospital in Nellore district, state of Andhra Pradesh, India.
As part of my continuing medical education, I chose a stroke center located in the Stroke Belt to visit and observed a comprehensive stroke care team in action. Here, I would like to share observations during my 2 weeks of a clinical preceptorship in cerebrovascular ultrasound and stroke management at the Comprehensive Stroke Center of the University of Alabama Hospital, Birmingham, AL.
Summary of Observations
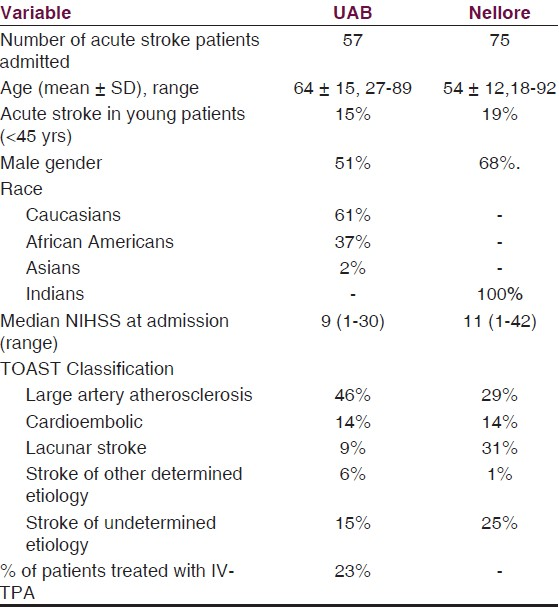
A total of 57 consecutive patients were admitted to the Stroke service. Their demographic characteristics, stroke severity, and subtypes are presented in Table 1. Comparative Figures for these characteristics of the stroke population admitted to my center in Nellore, India are also shown. Briefly, Nellore's stroke patients were younger, predominantly male and suffered from relatively severe strokes despite a higher proportion of lacunar subtype. Patients with large artery atherosclerosis constituted the commonest stroke subtype in Alabama, probable because of its being a tertiary care referral center.
Among patients with ischemic strokes and transient ischemic attack (TIA) at University of Alabama (UAB), all had structural imaging such as computerized tomography (CT) or magnetic resonance imaging (MRI) and at least one vascular imaging study (computerized tomographic angiography (CTA), magnetic resonance angiography (MRA), or cerebrovascular ultrasound).A total of 84% had a more comprehensive cerebrovascular imaging, which included either CTA or MRA and carotid/vertebral duplex with Transcranial Doppler (TCD). Of note, all patients undergoing carotid duplex also had TCD. The yield of carotid duplex in identification of a clinically-relevant mechanism of the disease was 84%, and the yield of TCD was 82%. In the presence of positive carotid duplex findings, TCD further provided relevant information in 60% of these cases.
In addition to non-invasive vascular imaging, 14% received diagnostic catheter angiography as part of completion of the diagnostic workup and planning for an intervention. Ultrasound findings were in agreement with catheter angiography in all, but 1 patient in whom an aberrant course of the posterior inferior cerebellar artery and diminutive vertebral artery produced an alternating and high resistance flow signals on Doppler. An overall agreement between catheter angiography and ultrasound was 83%.
Special investigations using different TCD techniques were done routinely.[3] The breath holding index test was done to assess the cerebral vasomotor reactivity, which aided in decisions on carotid revascularization and non-invasive ventilatory correction in reversed Robin Hood syndrome.[4] Bubble studies to detect a right-to-left shunt helped in diagnosing 2 patients having patent foramen ovale and pulmonary arterio-venous malformation as conduits for paradoxical embolism. Furthermore, TCD monitoring for emboli detection and during acute revascularization were performed nearly daily to assist with detection of recanalization and re-occlusion.
Although non-invasive vascular imaging is available at my center, they are under-utilized due to high cost and also due to lack of experience of the stroke team in performing and interpreting their results. I feel that the experience acquired here would largely change the mindset of my team.
8 out of 35 ischemic stroke patients received IV rt-PA (23% treatment rate). Those receiving IV t-PA were either treated remotely (phone-assisted “drip‘n’ship” t-PA administration at outside emergency rooms), or were on site using the combined lysis of thrombus in brain ischemia using transcranial Ultrasound and Systemic tPA (CLOTBUST-PRO)[5] or Argatroban tPA stroke study (ARTSS) protocols. Specifically, these protocols were designed to amplify rt-PA activity to induce and sustain an early recanalization. These patients were entered into the institutional review board (IRB) -approved clinical studies.
Furthermore, 7% of consecutive patients had emergent extra/intracranial revascularization procedures including angioplasty/stenting, thrombectomy with Penumbra™, and intra-arterial infusion of thrombolytics. Of note, interventionalists and cath lab personnel were on call 24 × 7, and these procedures were urgently performed any time, night, or day.
Due to late arrival of patients and high cost of treatment, only 3 patients received thrombolysis, and also due to lack of endovascular neuro-interventionalists, none of the interventions were performed at my center.
Every day, I witnessed proactive management of stroke patients based on “find reasons to treat” philosophy (as opposed to a more conservative way of “finding reasons not to treat,” common among our neurology colleagues, better known as “admiring the disability.”) Furthermore, daily discussions and investigations focused on identifying stroke pathogenic mechanism (as opposed to just localizing a lesion and disclosing prognosis) to institute early hemodynamic and ventilatory corrective measures as well as stroke mechanism specific secondary prevention measures. Finally, all patients with cerebral ischemia were getting an echocardiogram as well as telemetry.
As I mentioned before, UAB stroke center was also actively taking part in national institute of health (NIH) funded clinical trials like SAMMPRIS (stenting and aggressive medical management for preventing recurrent stroke in intracranial stenosis),[6] CUFFS (safety study of external counter pulsation as a treatment for acute ischemic stroke), and ARTSS (argatroban tPA stroke study).[7] A total of 6 patients were enrolled in these trials (3 ARTSS, 2 CUFFS, and 1 SAMMPRIS). Given an average rate of 0.5-1 patients/month worldwide enrollment into acute trials, I attribute the observed rate to dedication, availability of clinical research coordinators and sonographers 24 × 7, avoidance of “cherry picking,” and approaching all patients for participation if they met inclusion criteria for a given clinical trial.
As I take on a challenge to build a stroke team at my own hospital, I found the following useful. 24 × 7 × 365 stroke service consistently finding reasons to treat and applying the concept of time is brain and flow is brain regularly in all the cases. Although it appears very challenging, I plan to bring home and build a similar system open to patients’ access and capable of rapid delivery of stroke care.
I am extremely grateful to Prof. Andrei V. Alexandrov, director of the Comprehensive Stroke Center for giving me an opportunity to visit; and I admire this state of the art stroke service offered by him and his team in addition to teaching, training, and research. I would like to extend my acknowledgement to the residents Tim Prestely, Benjamin Ditty, Asad Chaudhary; interventionalists Damon Patterson, Mark Harrigan, Joseph Horton; sonographers Alice Robinson and Limin Zhao; clinical trial coordinator April Sisson; and research fellows Clotilde Balucani and Kristian Barlinn.
Source of Support: Nil
Conflict of Interest: None declared
References
- National Heart, Lung, and Blood Institute. In: Data Fact Sheet: The Stroke Belt: Stroke Mortality by Race and Sex. Hyattsville, Md: Dept of Health and Human Services; 1989.
- [Google Scholar]
- Birth and adult residence in the Stroke Belt independently predict stroke mortality. Neurology. 2009;73:1858-65.
- [Google Scholar]
- Cerebrovascular ultrasound in stroke prevention and treatment (2nd ed). New York: Wiley-Blackwell; 2011.
- Reversed Robin Hood syndrome in acute ischemic stroke patients. Stroke. 2007;38:3045-8.
- [Google Scholar]
- Design of a PROspective multi-national CLOTBUST collaboration on reperfusion therapies for stroke (CLOTBUST-PRO) Int J Stroke. 2008;3:66-72.
- [Google Scholar]
- SAMMPRIS Investigators.Design of the stenting and aggressive medical management for preventing recurrent stroke in intracranial stenosis trial. J Stroke Cerebrovasc Dis. 2011;20:357-68.
- [Google Scholar]
- Argatroban tPA stroke study: study design and results in the first treated cohort. Arch Neurol. 2006;63:1057-62.
- [Google Scholar]




