
Translate this page into:
Craniorachischisis totalis
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Neural tube defects (NTD) are common, severe congenital malformations resulting from complete or partial failure of the neural tube to close in the developing embryo. Anencephaly and spina bifida are important factors in fetal and infant mortality.[1] Each year, in the United States, approximately 4000 fetuses are affected, at least one third of them lost as a result of spontaneous or elective abortion.[2] All infants with anencephaly are stillborn or die shortly after birth. There is now strong epidemiologic evidence that a relative folate deficiency in the periconceptual period is causally related to many cases of NTD.[3] The incidence of anencephaly and spina bifida is usually higher in groups with lower socioeconomic status and at least half the cases of neural-tube defects can be prevented if women consumed sufficient amounts of the folic acid before conception and during early pregnancy.[4]
We report on a female fetus with craniorachischisis totalis. The fetus was of 13 weeks of gestational age, the crown rump length measured 118 mms. The fetus had anencephaly and spina bifida [Figure 1], the brain and calvaria were absent. In addition to these anomalies, it had exomphalos and sternal cleft [Figure 2]. The fetus went for spontaneous abortion at a rural hospital of Kerala state in South India. The detailed obstetric history of the mother was not available. Craniorachischisis, which combines anencephaly and total spina bifida with meningomyelocele, is the extreme example of defective neural groove closure. NTDs are usually multifactorial. To date, a few specific environmental causes of NTDs have been recognized, except for relatively rare sources of exposure such as maternal diabetes and maternal use of some antiepileptic drugs, such as valproic acid.[5]
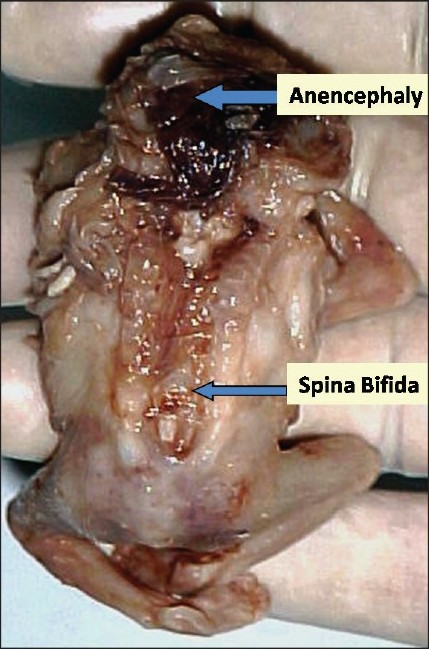
- Shows total craniorachischisis in the fetus of 13 weeks of gestational age (crown rump length – 118 mms)

- Shows the sternal cleft and examphalos in the same fetus, with total craniorachischisis
NTDs can be classified as open if neural tissue is exposed or covered only by membrane and closed, if the defect is covered by normal skin.[6] In anencephaly, the absence of the brain and calvaria can be total or partial. Craniorachischisis is characterized by anencephaly accompanied by a contiguous bony defect of the spine and exposure of neural tissue. In open spina bifida, a bony defect of the posterior vertebral arches (in this case, there was total anencephaly and open bifid spine was present throughout the vertebral column) is accompanied by herniation of neural tissue and meninges and is not covered by skin. In closed spina bifida, unlike open spina bifida, the bony defect of the posterior vertebral arches, the herniated meninges and neural tissue are covered by skin. Spina bifida occulta occurs most often at S1, S2, or both and is a bony defect of the spine, usually covered by normal skin. A meningocele is a saccular herniation of meninges and cerebrospinal fluid through a bony defect of the spine. Meningoceles are usually covered by normal skin. A myelomeningocele is the most common type of spina bifida and is characterized by herniation of the spinal cord, nerves, or both through a bony defect of the spine. Myelomeningoceles are usually open defects in which either meninges or neural tissues are exposed to the environment of these three types, only meningocele and myelomeningocele are typically included in studies of spina bifida and are often jointly referred to as spina bifida cystica. The spinous cleft is more common in the lumbar spine, may occur anywhere along the spinal column. In this case there is total spinous cleft and also there is anencephaly [Figure 1]. These defects are due to the failure of neural tube closure during development, preventing muscle and bone from growing around the gap.[7]
The development and closure of the neural tube are normally completed within 28 days after conception,[8] before many women are aware that they are pregnant. It is generally accepted that neural-tube defects are caused by the failure of the neural tube to close, although it has also been suggested that a closed tube may reopen in some cases.[9] To create the neural tube, the embryonic neural folds undergo major morphological changes, elevating from a semi-horizontal to a vertical position, and shifting from convex to concave, so that their tips, which were formerly pointed away from the midline, tilt towards the midline, touch and fuse. In nearly all the mouse NTD mutants examined, the exencephaly (the equivalent of human anencephaly), spina bifida (aperta) or rachischisis arise from failure to complete the process of elevation of the neural folds to become vertical and concave and thus they do not make contact to fuse and form a tube.
The embryologic basis of the clinical variation in NTDs is poorly understood. It has been proposed that in humans, as in mice,[10] closure of the neural tube occurs at several sites and that the clinical types of NTDs differ depending on the site at which closure fails.
Craniorachischisis is a congenital malformation which arises from incomplete closure of neural tube during early embryogenesis. Medical termination of pregnancy is advised if diagnosed early, since survival is not possible. Evidence strongly suggests that a substantial portion of NTDs, malformations of the developing brain and spinal cord, are due to a folate deficiency and can be prevented. Parental counseling and folic acid supplement, started before conception and continued through out the pregnancy are the recommended preventive measures. It is advised that women capable of becoming pregnant should consume 400 μg of folic acid per day.
References
- Central nervous system abnormalities--contrasting patterns in early and late pregnancy. Clin Genet. 1978;13:387-96.
- [Google Scholar]
- Centers for Disease and Prevention (CDC). Recommendations for the use of folic acid to reduce the number of cases of spina bifi da and other neural tube defects. MMWR Recomm Rep. 1992;41:1-7.
- [Google Scholar]
- Diet. In: Elwood JM, Little J, Elwood JH, eds. In. Epidemiology and control of neural tube defects (1st ed). Oxford, England: Oxford University Press; 1992. p. :521-603.
- [Google Scholar]
- Medical Research Council Vitamin Study Research Group. Prevention of neural tube defects: Results of the medical research council vitamin study. Lancet. 1991;338:131-7.
- [Google Scholar]
- The aplastic hypoplastic lumbar pedicle. Am J Roentgenol Radium Ther Nucl Med. 1974;122:639-42.
- [Google Scholar]
- Mechanisms of neural tube closure and defects. Metab Reta Dev Dis Res Rev. 1998;4:247-53.
- [Google Scholar]
- The pattern of neural tube defects created by secondary reopening of the neural tube. J Child Neurol. 1990;5:336-40.
- [Google Scholar]
- Neurulation in the mouse: Manner and timing of neural tube closure. Anat Rec. 1989;223:194-203.
- [Google Scholar]




